Implant software
Implant software
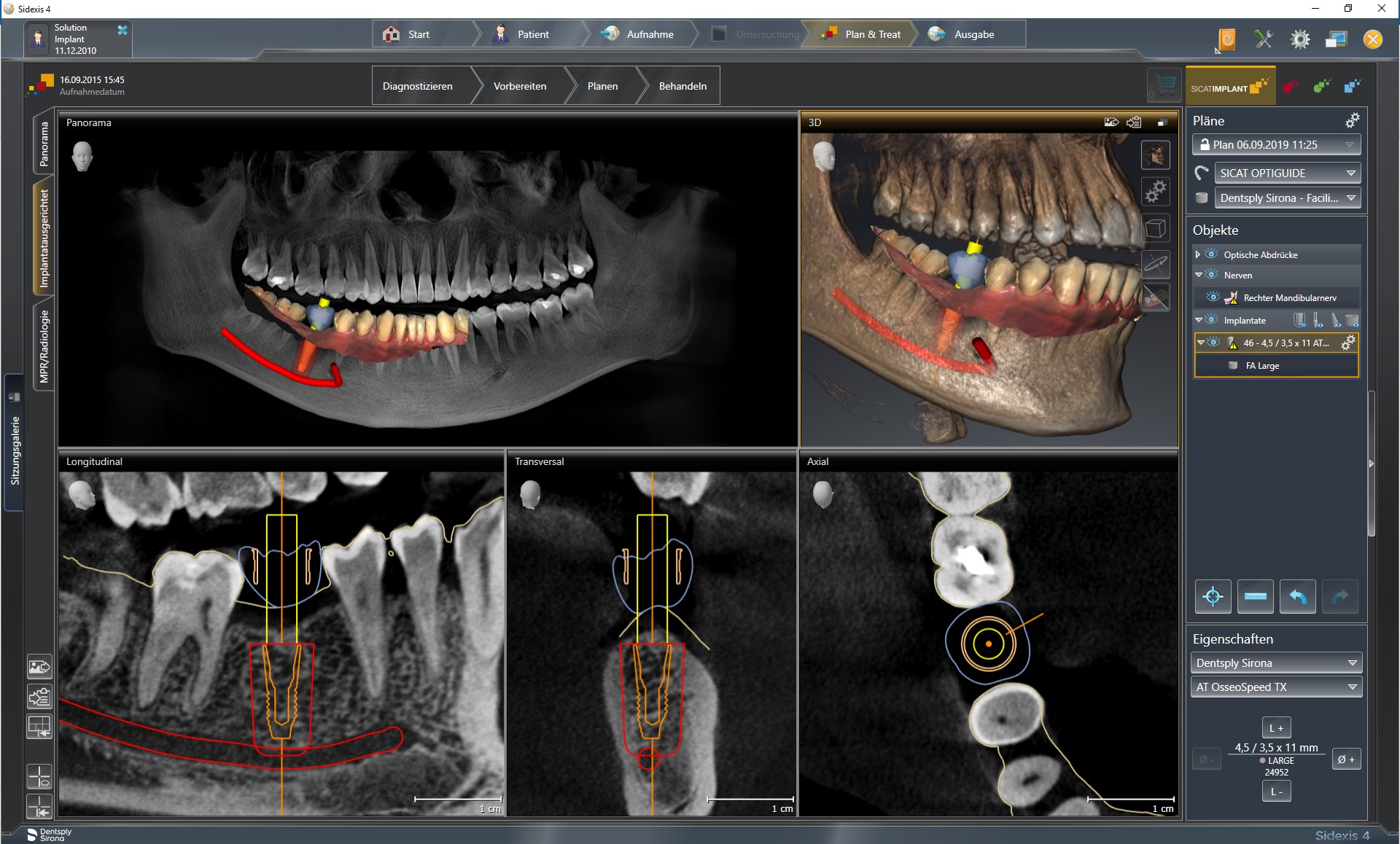
The use of implant software (for diagnostics and digital planning of implants) is a link in the digital processing chain and follows imaging procedures. It can process 2D and 3D X-ray data (from digital orthopantomographs, CTs or CBCTs) as well as clinical data scanned with intraoral scanners and visualise it with integrated viewer programmes. Apart from extremely precise, distortion-free images (including clear alignment of structures by overlapping partial images), aids such as scanbodies of known 3D geometry are also essential for transferring dimensions reliably. The image can be rotated three-dimensionally as required and flat (cross-sections) or curved 2D views calculated. Important structures (such as the mandibular canal) can be coloured in 3D images. Measuring instruments can be faded in for determining distances or angles thus making implant software suitable for preoperative diagnostics (bone volumes, bone quality, arrangement of important anatomical structures).
For backward planning, implant software can be used for achieving prosthetic objectives (e.g. by fading set-ups or wax-ups of the planned prosthetic restoration into the scan) by defining the parameters for implants and bone availability and evaluating whether augmentation is necessary.
Datasets of frequently used implants and abutments from virtual libraries stored in the implant software can be embedded in the optical three-dimensional image. This permits realistic planning of the number, dimensions (length, diameter), positioning and alignment of the implants.
 Implant software
Implant software
When implant software is used in conjunction with additional CAD programmes or modules, which include virtual teeth, occlusal surfaces, connectors and other prosthetic elements, the prosthesis can be planned entirely digitally. Together with CAM procedures, preoperative fabrication of (bone, tooth or mucosa supported) drilling templates with sleeves for guiding the drill during navigated implantation, custom abutments, temporary or even definitive superstructures is feasible.
One important demand placed on implant software is import/export compatibility (interfaces) with common data formats (such as Dicom and STL standard open formats). Proprietary systems with in-house formats are either tied to these (isolated applications) or can convert them to other (open) formats. In order to process the large datasets imported/exported by implant software, computer systems must possess sufficiently high data processing capacity and speed.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| dysmorphologic | dysmorphologisch |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration