Crowns
Crowns
Partial crowns or full crowns replace the outer layer of teeth, at least the enamel section, but also often to some extent large areas of dentine. If they are mainly fabricated for replacing lost tooth structure (tooth conservation), they can be considered a part of conservative dentistry but they often function as a component of restorations.
Crowns can be fitted on natural teeth (preparation) or the intraoral sections and abutments of implants. Crowns are retained by cementation and/or adhesion; it is also possible to fabricate screw-retained restorations on abutments. The long-term seal of the crown margin (marginal integrity) is very important for maintaining the health of the surrounding marginal periodontium and prevention of secondary caries.
 Anterior crown preparations
Anterior crown preparations
 Implant-borne metal-ceramic crown
Implant-borne metal-ceramic crown
Crowns are fabricated using a single material (full cast crown, all-ceramic crown) or by the combination of different materials (e.g. bonded crown). Very different procedures are used for this, e.g. casting (cast crown), milling, trimming, sintering (CAD-CAM), pressing (press-ceramic crown) or electroforming (electroformed crown). With a metal-ceramic crown a coping (framework) is first fabricated using metal and then coated with ceramic (veneered) to achieve optical similarity with the tooth. Historical techniques include soldering of crown parts (banded crowns).
 Three metal full cast crowns
Three metal full cast crowns
Prefabricated steel crowns can be used for treating severely destroyed deciduous teeth. Temporary (short, medium or long-term) custom-adapted prefabricated, frequently intraorally (direct) or extraorally fabricated temporary crowns (mainly using resins) bridge the period until a permanent crown is fitted.
Crowns fulfil various functions. As protective crowns they absorb masticatory forces to prevent teeth with weakened structures breaking apart and/or seal endodontically treated teeth against penetration of bacteria. They also protect the tooth against chemical and thermal irritation.
Anchor or abutment crowns retain bridges whereas support crowns anchor retentive and support elements such as rests and clasps. Connectors, e.g. attachments can also be integrated into the crown (attachment crowns).
Crowns can be fabricated individually (single crowns) or connected with other crowns (splinted crowns).
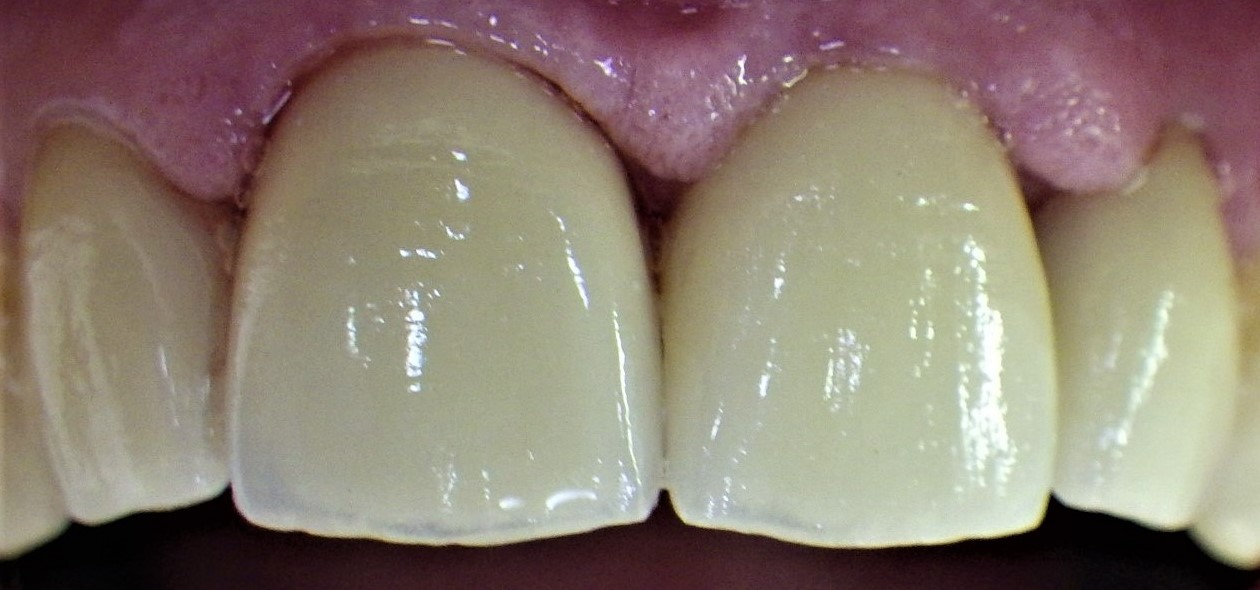 Upper anterior crowns
Upper anterior crowns
In the specific case of the telescope crown (conical telescope crown, parallel telescope crown) the crown consists of a fixed inner crown (primary crown) and an outer crown (secondary crown), which fits on the primary crown in the removable restoration. If a telescope crown is fabricated using the electroforming technique, it can be adhesively retained later in a tertiary crown fabricated over it.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| single-use system | Einwegsystem |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration