Spray mist ejection
Spray mist ejection
In modern dentistry water sprayed from nozzles, e.g. in handpieces, is used for a wide range of applications, in particular for cooling, rinsing and cleaning as well as an enveloping, binding medium such as for ultrasonic cavitation, polishes or abrasives.
 Spray mist ejector
Spray mist ejector
When compressed air is added and the water collides with rapidly rotating instruments, so-called "spray mist", i.e. (mostly contaminated) aerosols are created. They consist of finely distributed water droplets ("mist") which surround the patient's mouth up to a radius of 1.5 m during, and for some time following, the treatment. Spray mist also contains a large number of further constituents such as solid particles from the various materials employed in and reduced from the mouth and tooth structure as well as liquids such as saliva or blood containing all types of pathogen (bacteria, viruses, fungi). Although no longer visible, when atomised to form a "cloud", the minute single droplets are especially apt at contaminating surfaces of objects in the surgery, the skin of persons in the vicinity or for being inhaled ("aspirated"), swallowed or absorbed via membranes, e.g. the eyes.
Where spray mist is concerned, the most important objective of dental hygiene, i.e. avoiding contamination and preventing cross-contamination, is achieved by providing surgery staff with passive protection via a mouth/nose mask and protective glasses. The stream of air/water is guided accurately and extracted which ensures that all constituents are removed as completely as possible from the mouth immediately after being released, which shrinks the "spray mist cloud" considerably but without compromising the desired effects.
Within a few years of high speed, water-cooled dental handpieces being invented in the mid-20th century, suitable suction devices such as a mobile suction pump (1955) and a suction unit specifically designed for extracting spray mist when treating reclined patients (1961/1964) were developed.
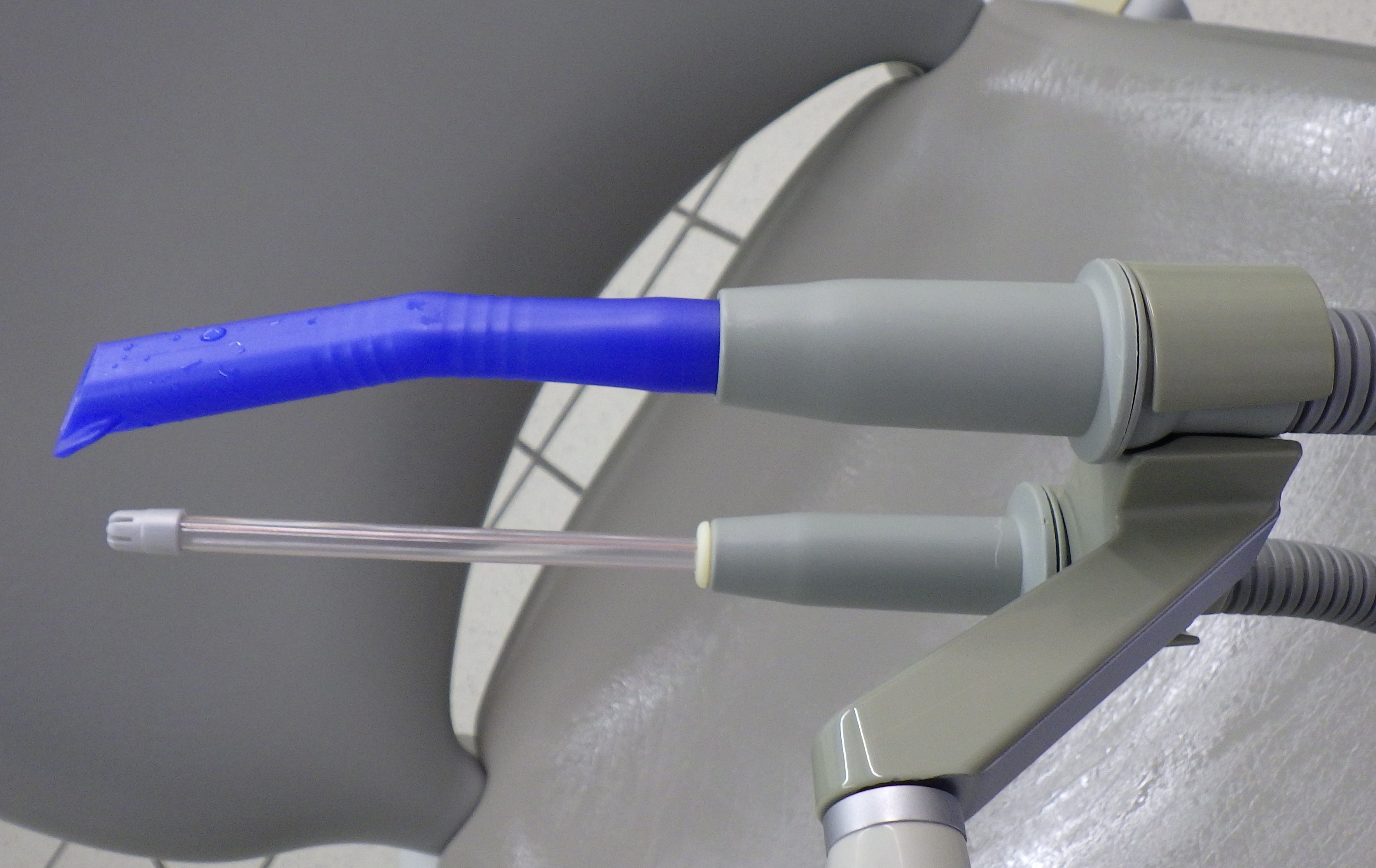
 Spray mist ejector viewed from above
Spray mist ejector viewed from above
Modern spray mist extractors include integral or external modules for separating air, water and solids (such as amalgam particles). The flow rate ranges from several hundred to one thousand l/min. Innovative technology (for example, the radial motor or electronic controller) greatly reduces the required space, energy consumption and noise level. Whereas previously "suction machines" were installed in the basement, nowadays they can be used in close proximity to the treatment zone.
The suction effect generated in dental units is applied via flexible suction hoses (some can be adjusted or closed off with slider valves) with adapters for fitting rigid, standard diameter (mostly 16 mm for spray mist) saliva ejectors which are normally for multiple-use and autoclavable. The ejectors (available in different sizes for children and adults) include gripping surfaces and their ends are usually formed like a flat pelotte for holding back soft structures. To prevent suck-back of liquids if the ejector becomes totally blocked it may include permanently open side air-inlets. Suction hoses for surgical purposes (often with sterile, disposable cannula) or saliva ejection (often with non-sterile disposable cannula) usually have smaller diameters.
Regular rinsing, cleaning and disinfection of the entire suction system using purpose-made, non-corrosive solutions is an important measure for avoiding blockage, damage and formation of contaminated biofilms (germ colonisation).
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| add facings | verblenden, Verblendprozess |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration