Röntgen
Röntgen
Die nach Wilhelm Conrad R. (dt. Physiker, 1. Physik-Nobelpreis 1901) benannten nicht sichtbaren R.-Strahlen (zunächst "X-Strahlen", engl. noch heute "X-rays") dienen zu therapeutischen, überwiegend aber zu diagnostischen Zwecken in Medizin, Zahnmedizin, Substanz- und Materialprüfung.
Die elektromagnetische (ionisierende, also ungeladene Moleküle in Ionen und Elektronen zerlegende) R.-Strahlung hat kürzere Wellenlänge als das sichtbare Licht. Sie durchdringt Körpergewebe und ist biologisch schädlich, so etwa karzinogen (krebserzeugend), mutagen (erbgutverändernd) und teratogen (Schädigung des Embryos). Deshalb müssen zur Minimierung der Strahlenbelastung die Häufigkeit (etwa die Zahl von R.-Aufnahmen) und die jeweilige Einzeldosis auf das absolut Notwendige beschränkt werden. Bereiche, die nicht bestrahlt werden sollen, sind mit geeigneten Materialien (meist Blei, etwa in R.-Schilden, R.-Schürzen, R.-Schutztüren, etc.) abzuschirmen.
Die Beugung von R.-Strahlen lässt Rückschlüsse auf die Struktur von Molekülen (DNA), Kristallen und Materialien zu. Die Abgabe von elementtypischen Spektren von R.-Strahlung nach Bestrahlung mit Elektronen oder R.-Strahlen (R.-Fluoreszenz) ermöglicht die Analyse der in Stoffen enthaltenen chemischen Elemente.
Mit R.-Strahlung können orthopädische Schmerzzustände ("R.-Entzündungsbestrahlung") und strahlenempfindliche Tumorzellen bekämpft werden. Die (z.B. intraoperative) Durchleuchtung von Körperstrukturen (mittels R.-Bildverstärkern) dient der Analyse von Abläufen und Optimierung (z.B. Reposition von Frakturen).
Anlässe für diagnostische R.-Aufnahmen können akute Beschwerden, Traumata oder Erkrankungszustände sein, aber auch Ausschluss und Frühdiagnose von Schäden (Bissflügel-R. zur Kariesfrüherkennung) sowie Planung und Verlaufskontrolle zahnärztlicher Behandlungsmaßnahmen (Chirurgie, Endodontologie, Implantologie, Kieferorthopädie, Prothetik).
 Ausgedehnte kariöse Kavität an 27
Ausgedehnte kariöse Kavität an 27
 Zahnfilm, Kleinröntgenaufnahme
Zahnfilm, Kleinröntgenaufnahme
In der Zahnheilkunde werden selten intraoral, meist jedoch extraoral angeordnete R.-Röhren (R.-Strahler) eingesetzt, um analoge, lichtempfindliche R.-Filme (chemische Entwicklung und Fixierung in der Dunkelkammer), R.-Speicherfolien (Anregung von Leuchtstoff, Abtastung mittels Laser) oder digitale R.-Sensoren (CCD- oder CMOS-Halbleiterbauelemente) zu bestrahlen. Die R.-Spannung der verwendeten "konventionellen" R.-Strahlung liegt bei 60 bis 70 Kilovolt. Mit ruhenden Geräten werden zweidimensionale Aufnahmen (Zahnfilm, Fernröntgenseitenbild, Kiefergelenkaufnahme), mit rotierenden Systemen Schichtaufnahmen (Orthopantomogramm) und dreidimensionale Aufnahmen (CT = Computertomografie, DVT = Digitale Volumentomografie) erstellt. Die Betrachtung erfolgt auf R.-Bildbetrachtern (analog) oder (ggf. verbunden mit Bildbearbeitung) am Computermonitor (digital).
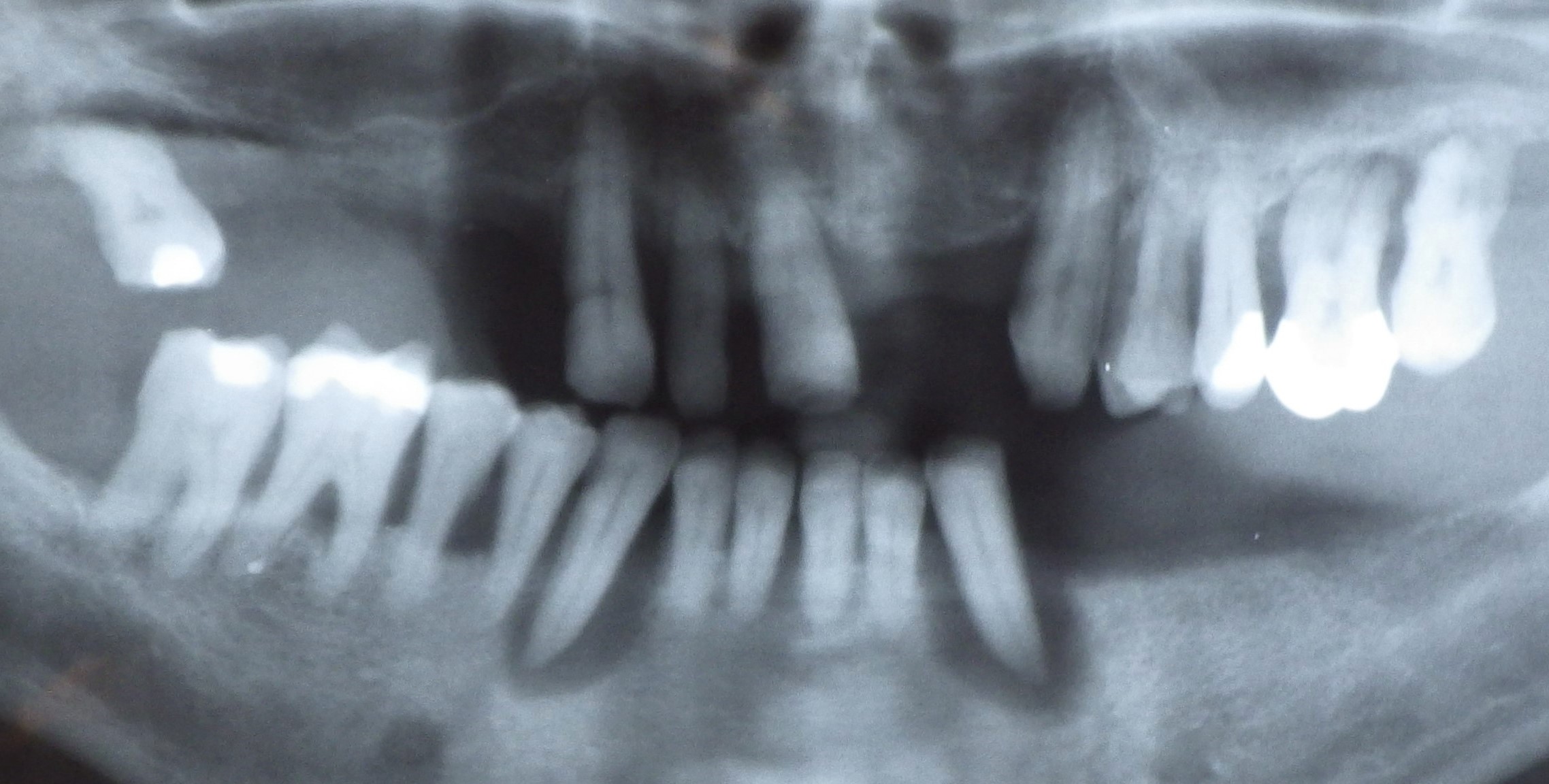 Panoramaaufnahme, Orthopantomogram
Panoramaaufnahme, Orthopantomogram
 Orthopantomogramm eines 8-Jährigen (Wechselgebiss)
Orthopantomogramm eines 8-Jährigen (Wechselgebiss)
Verschiedene Körpergewebe enthalten unterschiedlich große Mengen chemischer Elemente, deren Protonenzahl im Atomkern und damit deren Schwächung (Absorption) der R.-Strahlung sich unterscheidet, was sich als Bildkontrast, etwa zwischen Hartsubstanzen mit unterschiedlichem Calciumgehalt (Knochen, Dentin, Zahnschmelz) und Weichgewebe zeigt. Es entsteht ein Graustufenbild mit einer Auflösung von bis zu 20 Linienpaaren pro Millimeter oder 25 µm. Die übliche Negativdarstellung führt zu entsprechend "umgekehrter" Terminologie, hellere Bereiche werden als Verschattung, dunklere als Aufhellung bezeichnet.
In den Mundraum eingebrachte Fremdkörper aus Metall (Amalgam, Guss-Restaurationen) und Keramiken weisen in der Regel hohe "R.-Opazität" ("Undurchsichtigkeit") auf und erscheinen weiß oder hellgrau.
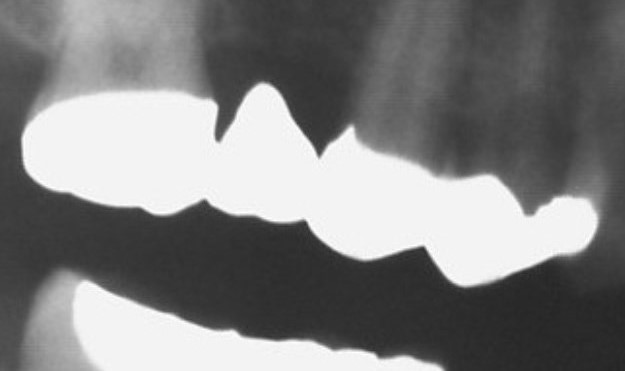 Brückenersatz 16 (Brückenglied) Ankerkronen 17 + 15
Brückenersatz 16 (Brückenglied) Ankerkronen 17 + 15
Füllungsmaterialien (provisorische Verschlussmasse, Komposit und Guttapercha) Medikamente (Calciumhydroxidpaste) oder Kunststoffe und Prothesenzähne für R.-Schablonen können mit positiven R.-Kontrastmitteln r.-sichtbar ("radio-opak") gemacht werden.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| interior of a crown | Kroneninnenfläche, Kroneninnenseite, Kroneninneres, Kronenlumen |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration