Implantat
Implantat
Dentalimplantate sind künstliche, vorwiegend zahnwurzelähnliche (zylindrische oder konische) Strukturen zur Insertion in den Knochen. Sie dienen vor allem zur intraoralen Verankerung von festsitzendem oder herausnehmbarem Zahnersatz (Suprakonstruktion), in speziellen Fällen auch von kieferorthopädischen Apparaturen oder Defektprothesen (Epithesen).
Implantate des 21. Jahrhunderts bestehen selten aus Zirkoniumdioxid, meistens aus Reintitan. Dieses leichte und stabile Metall ist bioinert, eine An- und Einlagerung von Knochen ist so möglich. Für die dauerhafte Stabilität bei funktioneller Belastung von Implantaten ist eine starre Fixierung des Implantates durch spaltfrei anwachsenden Knochen, die so genannte Osseointegration, von entscheidender Bedeutung. Das Einwandern lebender Knochenzellen und das Einwachsen von Knochen in die Implantatoberfläche werden durch geeignete Verfahren zur Aufrauhung, Nischenbildung und Oberflächenvergrößerung erleichtert. Dies gilt auch für den Implantathals, der nur zu Beginn der Entwicklung glatt poliert gefertigt wurde.
Zur Vorbereitung der Implantation erfolgen zunächst dünne Bohrungen im Knochen, die mittels weiterer Bohrer (vor allem in kompaktem Knochen) und/oder Instrumenten zur Knochenverdichtung (vor allem in spongiösem Knochen) steigenden Durchmessers schrittweise bis zum angestrebten Enddurchmesser der Knochenkavität erweitert werden. Das manuelle oder maschinelle Einsetzen des zylindrisch-konischen Implantats mit Außengewinde(n) entspricht dem kontrollierten Eindrehen einer Schraube. Durch geringfügige Presspassung und selbstschneidende Gewinde kann häufig eine ausreichende Primärstabilität erreicht werden.
Der Oberrand des Implantats, die sogenannte Plattform, kann auf Knochenniveau oder auf Schleimhautniveau liegen.
 Titan-Implantate auf Knochenniveau
Titan-Implantate auf Knochenniveau
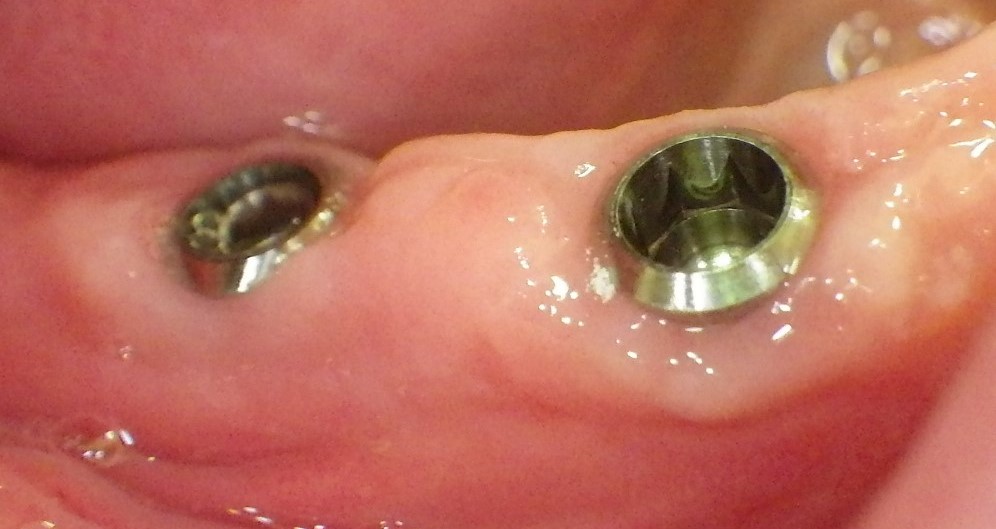 Implantate auf Zahnfleischniveau
Implantate auf Zahnfleischniveau
Die Einheilung erfolgt gedeckt (unter der darüber dicht verschlossenen Schleimhaut) oder offen (unter intraoperativer Ausformung eines Schleimhautkragens.)
Aufgrund von Knochenresorption nach Zahnverlust steht für Implantate oft weniger Knochenvolumen zur Verfügung. Dementsprechend werden Verfahren zum Knochenaufbau angewendet (etwa GBR), aber auch geringer dimensionierte (z.B. durchmesserreduzierte) Implantate eingesetzt. Übliche Implantate weisen einen Plattform-Durchmesser von etwa 4 mm auf, deutlich darüber liegende Maße werden als "wide", deutlich darunter liegende als "narrow" und noch dünnere Implantate als "Mini-Implantate" bezeichnet.
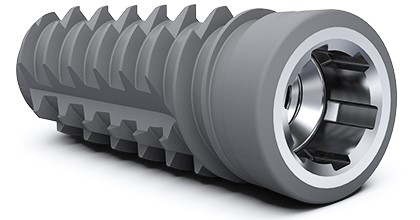
Moderne Dentalimplantate sind in der Regel zweiteilig. Implantat (Ersatz für die Zahnwurzel) und Aufbauteil werden dabei formschlüssig und kraftschlüssig verbunden. Durchgesetzt hat sich vor allem die Innenkonusverbindung mit zusätzlichen ineinandergreifenden "Nut- und Feder"-Elementen zur Rotationssicherung. Befestigungsschrauben werden mit definiertem Drehmoment angezogen, um Bewegungen, Lockerung und Materialüberlastung auszuschließen.
 Ein modernes Implantat
Ein modernes Implantat
Hatte früher das Abutment basal stets den Durchmesser der Implantatplattform, sind moderne Abutments an dieser Stelle oft geringer dimensioniert. Dieses sogenannte "platform switching" soll zu besserem Knochenerhalt führen.
 Ein Implantat der neuen Generation
Ein Implantat der neuen Generation
Für die natürliche Wirkung von implantatgetragenen Restaurationen (Rot-Weiß-Ästhetik) und gesunde periimplantäre Verhältnisse wird ein möglichst anatomisch korrektes Durchtrittsprofil (Emergenzprofil) angestrebt.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| speed | Drehzahl, Empfindlichkeit, Empfindlichkeitsklasse, Tourenzahl, Umdrehungszahl, Umdrehungen, Rotationsgeschwindigkeit |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration