Shade-taking for restorations
Shade-taking for restorations
Mimicking the positioning, contours and optical surface properties of adjacent and opposing natural teeth as realistically as possible is an important part of integrating dental prostheses inconspicuously into the mouth. The optical surface properties are summarized by the term "tooth shade" despite the fact that they include a wide range of parameters such as shade, shade gradient, brightness, shade saturation, translucency (light shimmering through light-scattering material) versus opacity (due to scattering of light), fluorescence or phosphorescence (light emission due to, e.g. UV light), glaze (due to reflection of light).
The virtually infinite spectrum comprising millions of naturally occurring tooth shades subjectively perceptible to the human eye can be reduced to a few standardised shades (clearly defined and described for objective documentation and communication) and only incur minimal aesthetic sacrifices. These are then incorporated into so-called shade guides (mostly one-dimensional/linear, rarely multi-dimensional, encompassing various parameters) such as for prefabricated denture tooth. These shade tabs are usually contoured like teeth, made of the restorative (e.g. composite or porcelain) and used for comparing with patients' teeth and/or restorations.

Shade guide
Shade guides are also available in gingival shades for imitating soft tissues such as mucosa.
As each specific surface appears differently (metamerism) when illuminated with light of differing intensities or wavelengths (sun, cloudy, dawn, artificial lighting), in order to achieve predictable results wherever possible shade-taking must be carried out under reproducible, standardised lighting conditions. To achieve these, various technical aids such as identical ring lights for dentist and technician, cameras with white balance or special electronic devices which measure spots or use standardised photos for "surveying" the various areas of the tooth (such as the incisal, dentine, cervical and proximal regions) and displaying the results to correspond with standard shade guides are employed.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| bone remodeling | Knochenremodellation, Knochenumbau, knöcherne Remodelling, Knochenremodelling |
Focus text of the month
Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication… Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication for root canal posts. The preferred method is generally to insert the root canal post, so that it (by predrilling with ascending diameters) virtually fills the prepared post site and fits close to the dentine wall. That section of the root canal post in the root should be at least as long as the crown restoration, leaving a few millimetres of the root canal filling to seal the apex. Isolated concepts have also been developed with smooth metal posts projecting apically beyond the tooth and intended for anchoring in the bone (transdental fixation).
Restoration with a temporary post is seldom practical due to the increased fracture and reinfection rate; a definitive root canal post should be inserted as early as possible.
Customised root canal posts (often made from precious metal alloys), cast after waxing up directly in the root canal or indirectly after taking an impression of the root canal lumen (using burnout posts), can also be used for filling lumina with oval or irregular cross sections, as well as two or three divergent canals each fitted with a post inserted, if necessary, through the opening of another canal. The core build-up(s), or even the entire crown (historically: post crown) can be integrated. |
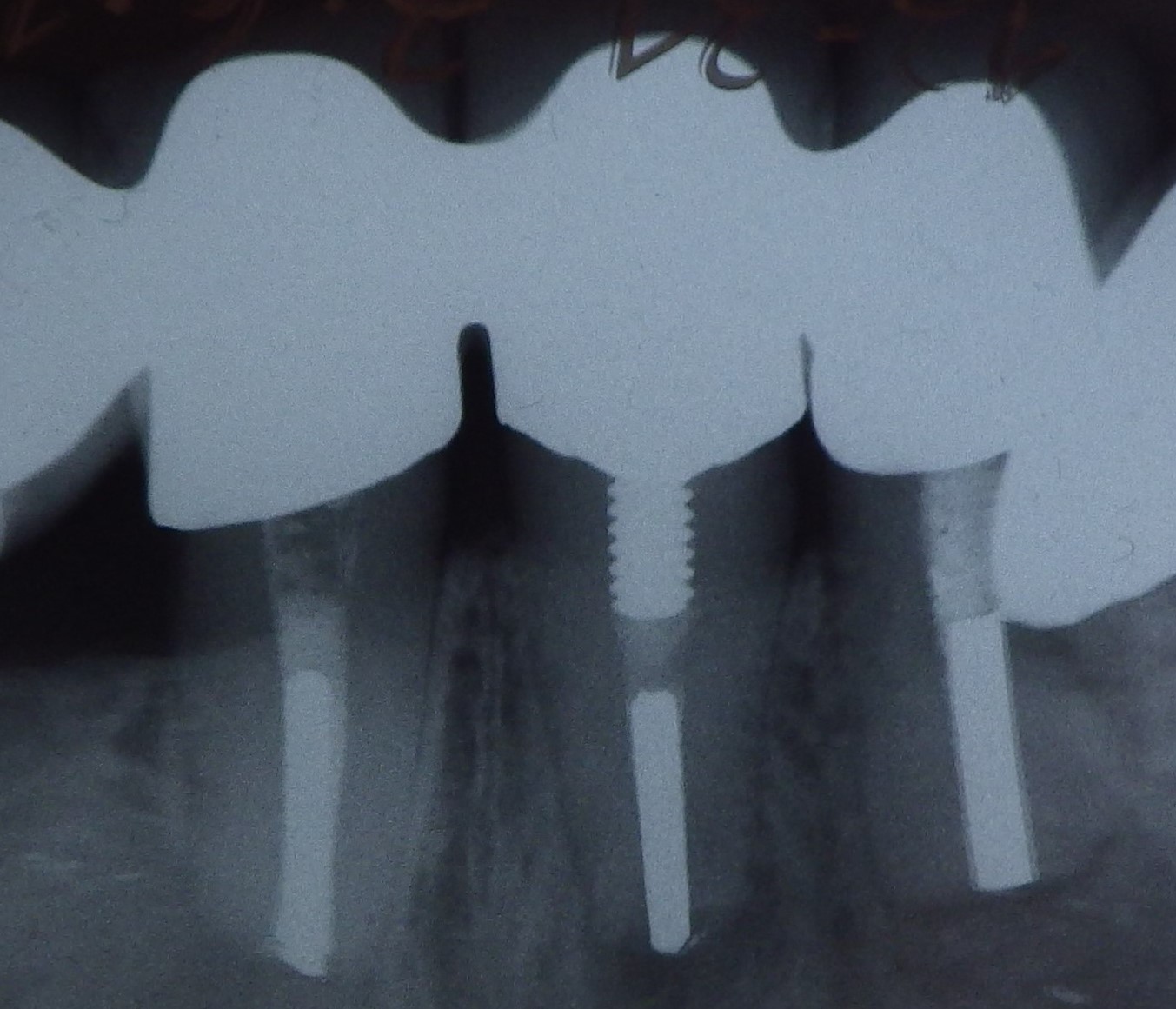 Three different root canal posts
Three different root canal posts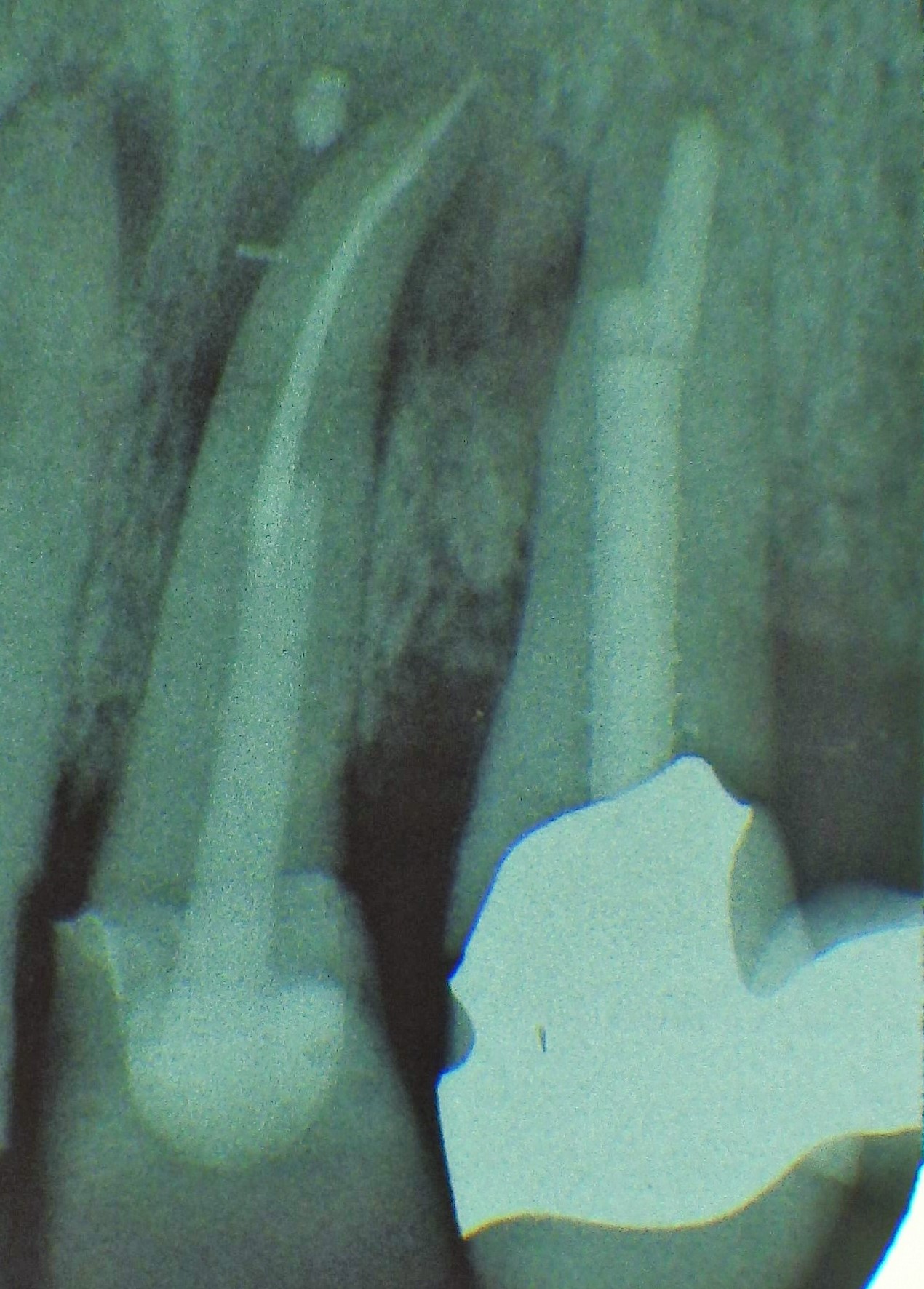 Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Tooth 14 conical and smooth, tooth 13 cylindrical and threaded