Impression materials
Impression materials
Dental impression materials are used for taking impressions in the mouth. They are intended for reproducing and transferring the outer contours of intraoral structures (teeth, jaws, soft tissues, fillings, restorations) three-dimensionally during impression-taking. An initially soft material is applied directly to the surface, avoiding air voids where possible, before setting rapidly (between one and a few minutes) in a supporting impression tray to create a female mould (impression). The impression is then cast (usually with plaster but possibly with acrylic resin) to produce a model.
In the past, plaster was used for taking impressions even though it was not elastic after setting. For this reason, a plaster impression of undercut structures (teeth) always had to be sectioned (fractured) in order to withdraw it from the mouth. Impression plaster was also used as a pick-up impression material for single-prep impressions taken using customised copper rings filled with thermoplastic (resin-based) impression material. However, after cooling and setting the rigid impression could not be removed from undercuts without being damaged.
For this reason, nowadays rigid setting, reversible thermoplastic materials are only used in non-undercut regions, e.g., resins for functional impressions on denture peripheries or waxes for bite registration.
Special zinc-oxide-eugenol impression materials may also be used when taking functional impressions.
For decades almost only impression materials which remain elastic after setting and, when sufficiently thick, virtually fully recover their original shape after removal from the mouth, have been in use. This property is referred to as “elastic recovery”.
These include alginate impression materials which, when mixed with water, form gel-like polysaccharides. As alginate impressions may dry out or absorb further water and swell, they are neither dimensionally stable nor can they be stored for longer periods. This also applies to reversible hydrocolloids.
In the meantime, so-called elastomeric alginates, which are generally irreversible materials and set to a rubbery-elastic consistency, are widely accepted. The chemistry behind the chain reactions can be divided into polymerization (e.g. polyether impression materials), polyaddition (e.g. A-silicones) and polycondensation (e.g. C-silicones, polysulfides). These impression materials are either mixed by hand or mechanically (refer to “Mixing systems for impression materials”) to combine two components (“base” and “catalyst”) homogeneously and void-free.
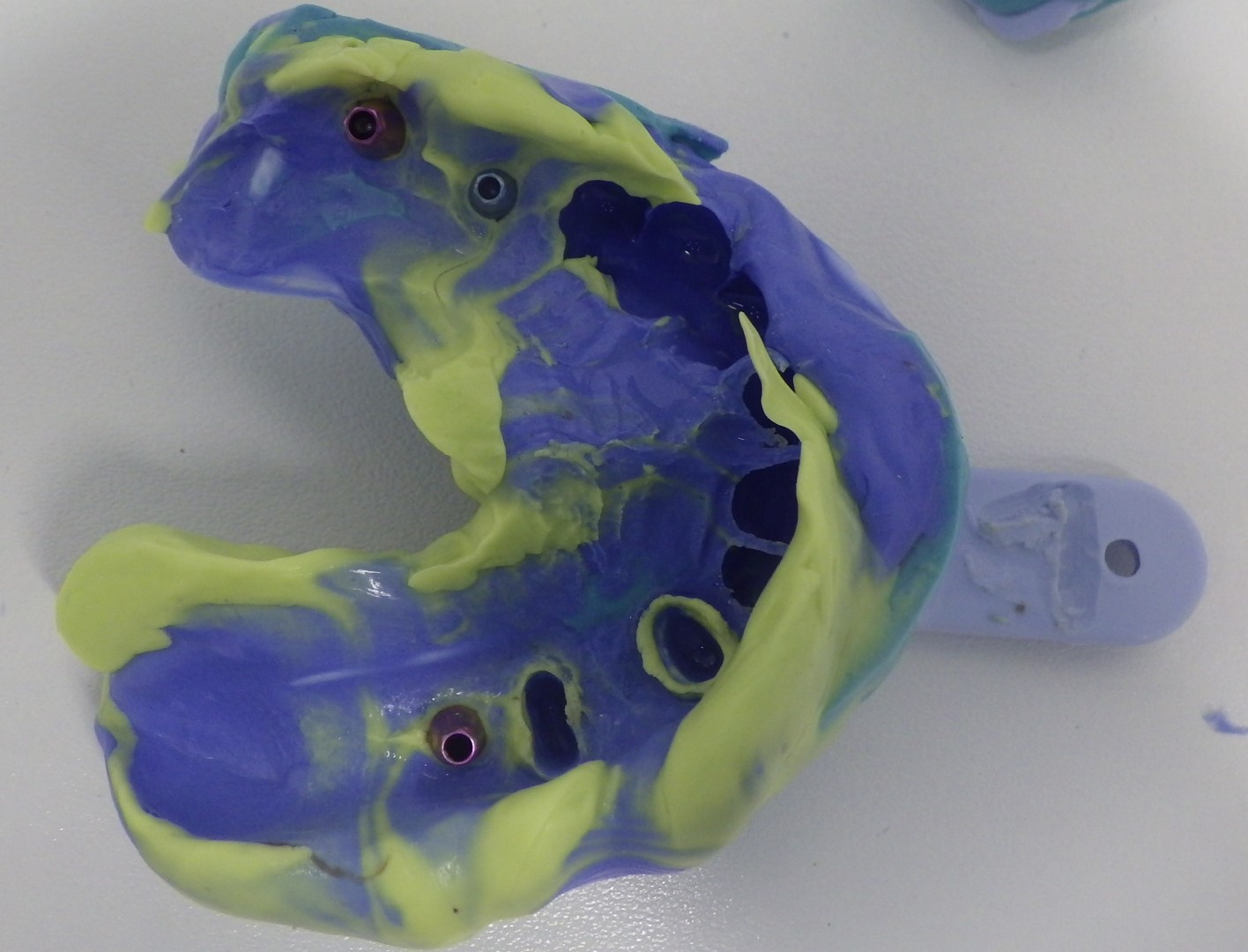 One-step putty-wash impression taken with regular and light body silicones over impression posts
One-step putty-wash impression taken with regular and light body silicones over impression posts
Silicone impression materials (polyvinyl siloxanes, PVS) in particular are supplied in different consistencies for various impression procedures. When taking one-step or two-step putty-wash impressions, a kneadable (heavy body) putty exerts controlled pressure (usually in an impression tray) on a syringeable, light body, low viscosity precision impression material. This allows it to penetrate narrow gaps (e.g., intraorally in the gingival sulcus, interdental spaces, fissures) thus increasing the accuracy of detail (crispness) of the precision impression.
Materials which are also kneadable yet slightly less viscous, and with an extended setting time, are used for taking functional impressions for full dentures. They intentionally displace very compressible mucosal areas more than firm sections (varying mucosal resilience) thus balancing the pressure exerted which reduces the risk of denture sores.
Regular body silicone impression materials are either used with other materials or alone (monophase) e.g., for taking pick-up impressions for fixed/removable restorations either involving implants or not.
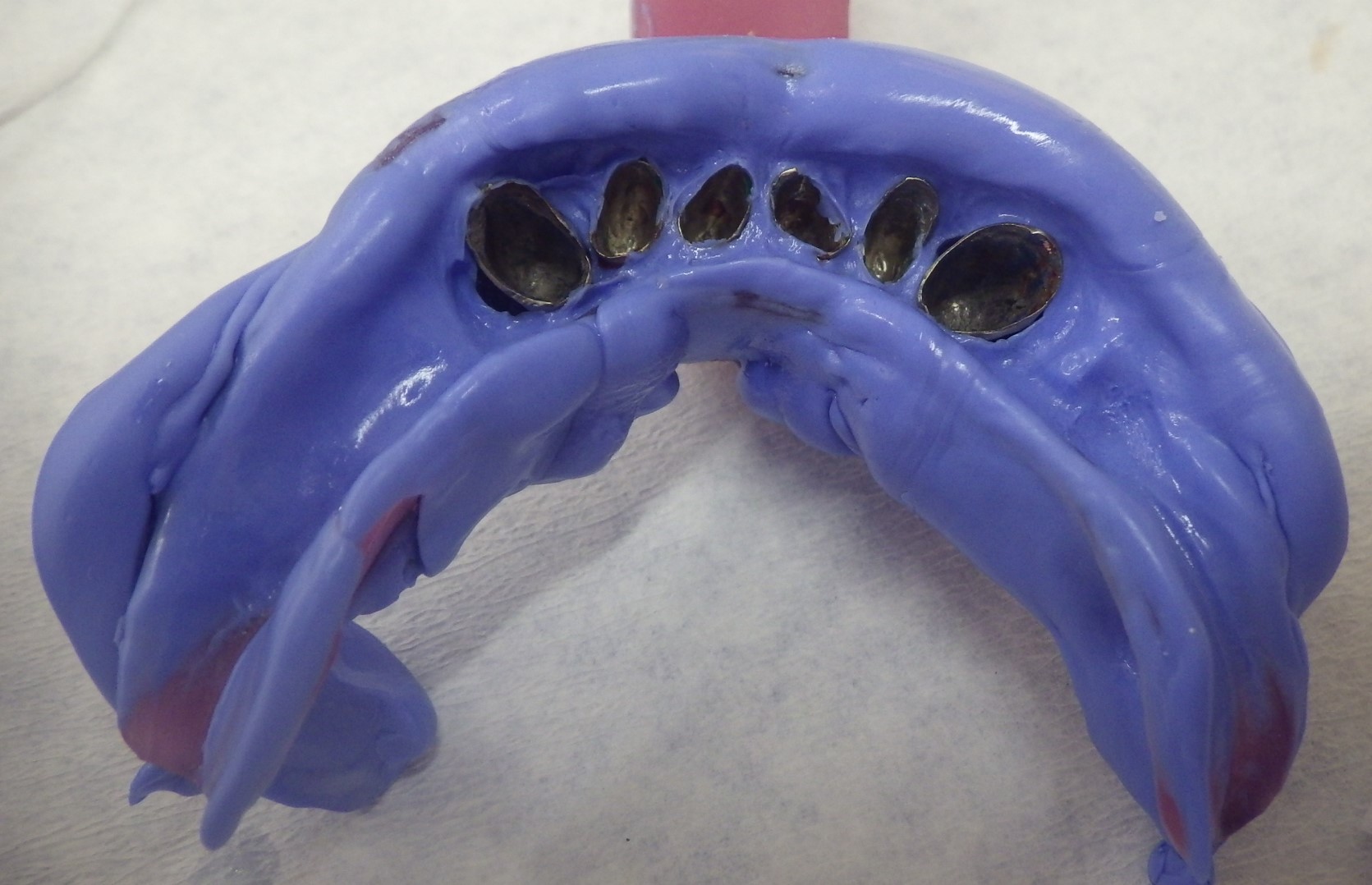 Pick-up impression taken over inner telescopes using monophase silicone
Pick-up impression taken over inner telescopes using monophase silicone
To ensure that the impression material flows smoothly onto surfaces, which are often moist, a degree of hydrophilicity (acute contact angle) is desirable.
The setting reaction of impression materials may be accelerated by specific additives or a warmer environment (e.g., intraoral) but can also be retarded by inhibitors or precooling. Processing encompasses the mixing time, working time (loading the tray with impression material and inserting it into the mouth) and setting time. Special chromatic impression materials change colour to indicate the changes.
Silicone impression materials which attain their final hardness very quickly can also be used for bite registration.
Nowadays, materials for analogue impressions are often no longer required as contactless optical procedures using intraoral scanners are increasingly in use (digital impression-taking).
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| porcelain application instrument | Keramikinstrument |
Focus text of the month
Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication… Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication for root canal posts. The preferred method is generally to insert the root canal post, so that it (by predrilling with ascending diameters) virtually fills the prepared post site and fits close to the dentine wall. That section of the root canal post in the root should be at least as long as the crown restoration, leaving a few millimetres of the root canal filling to seal the apex. Isolated concepts have also been developed with smooth metal posts projecting apically beyond the tooth and intended for anchoring in the bone (transdental fixation).
Restoration with a temporary post is seldom practical due to the increased fracture and reinfection rate; a definitive root canal post should be inserted as early as possible.
Customised root canal posts (often made from precious metal alloys), cast after waxing up directly in the root canal or indirectly after taking an impression of the root canal lumen (using burnout posts), can also be used for filling lumina with oval or irregular cross sections, as well as two or three divergent canals each fitted with a post inserted, if necessary, through the opening of another canal. The core build-up(s), or even the entire crown (historically: post crown) can be integrated. |
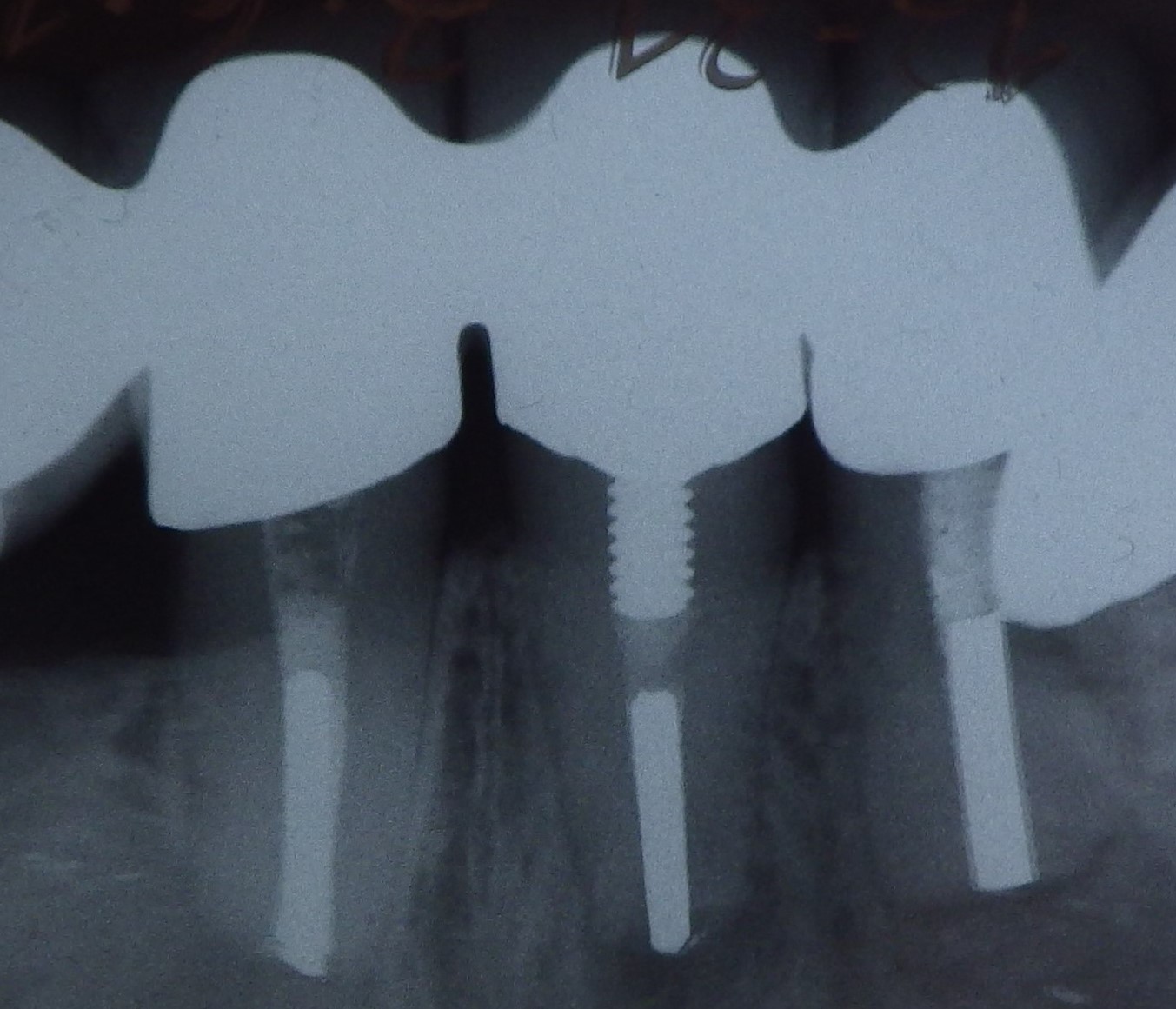 Three different root canal posts
Three different root canal posts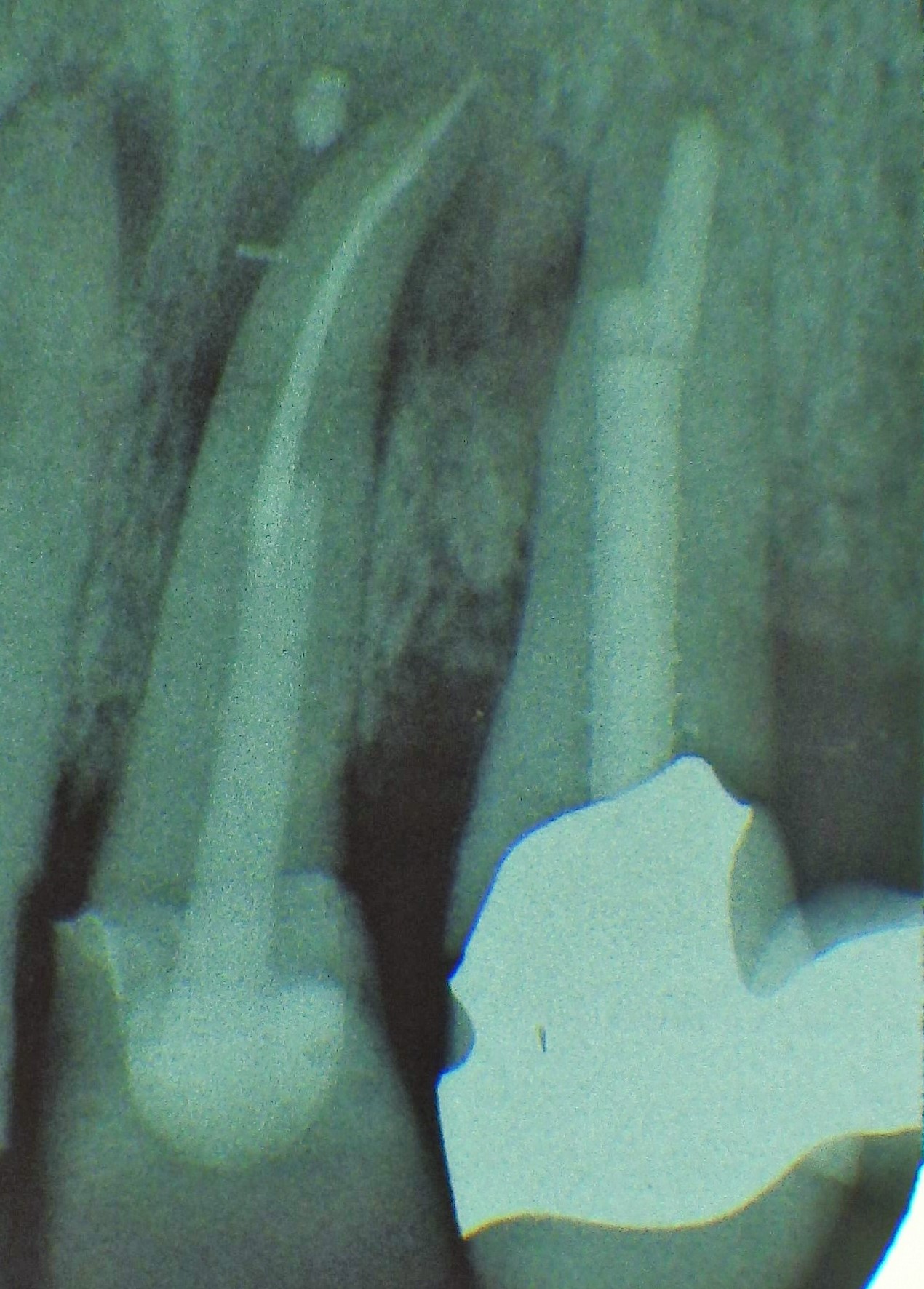 Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Tooth 14 conical and smooth, tooth 13 cylindrical and threaded