Porcelain furnaces
Porcelain furnaces
Modern, 21st century porcelain furnaces are technically sophisticated, electronically-controlled devices with programmable cycles for firing dental porcelains. These include metal-ceramics for firing onto metal frameworks (classic precious or non-precious alloys, titanium) or all-ceramics such as zirconia or lithium disilicate. All-ceramic inlays or laminate veneers can be fired directly onto refractory model dies.
The principle unit of a porcelain furnace is its refractory firing chamber. Once the porcelain has been built up, the restorations can be placed onto mesh, cones, pins or firing pads for firing.
The heating coils are usually located in the upper housing of the furnace and arranged concentrically around the restoration. A motor-driven mechanism closes the firing chamber with the restoration inside, either by raising the firing platform or lowering the upper housing of the furnace. The firing cycle settings depend on the material being fired/procedures and run according to pre-set, standardised or custom programmes.
Many settings can be programmed precisely and independently of each other, for example times can be set to the split second (preheating/drying, heat-rate, hold-time, cooling) and firing temperatures for various materials such as opaquer, shoulder and dentine porcelains as well as glaze firings programmed accurately.
As the only way of preventing undesirable opacity in the porcelain is to evacuate the firing chamber during firing (vacuum phase), a built-in powerful vacuum pump is an essential part of a porcelain furnace.
 Porcelain furnace
Porcelain furnace
Combined firing/pressing furnaces are used for fabricating pressed-ceramic restorations (pressing procedure resembling casting which makes use of pressure and heat to liquefy ceramic blocks and force them into lost, refractory investment moulds) using special firing chambers and pressure plungers.
Whereas glass infiltration firing of presintered ceramic is possible in a porcelain furnace ("infiltration firing"), special high temperature sintering furnaces are required for the actual sintering process (such as for zirconia).
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| porcelain application instrument | Keramikinstrument |
Focus text of the month
Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication… Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication for root canal posts. The preferred method is generally to insert the root canal post, so that it (by predrilling with ascending diameters) virtually fills the prepared post site and fits close to the dentine wall. That section of the root canal post in the root should be at least as long as the crown restoration, leaving a few millimetres of the root canal filling to seal the apex. Isolated concepts have also been developed with smooth metal posts projecting apically beyond the tooth and intended for anchoring in the bone (transdental fixation).
Restoration with a temporary post is seldom practical due to the increased fracture and reinfection rate; a definitive root canal post should be inserted as early as possible.
Customised root canal posts (often made from precious metal alloys), cast after waxing up directly in the root canal or indirectly after taking an impression of the root canal lumen (using burnout posts), can also be used for filling lumina with oval or irregular cross sections, as well as two or three divergent canals each fitted with a post inserted, if necessary, through the opening of another canal. The core build-up(s), or even the entire crown (historically: post crown) can be integrated. |
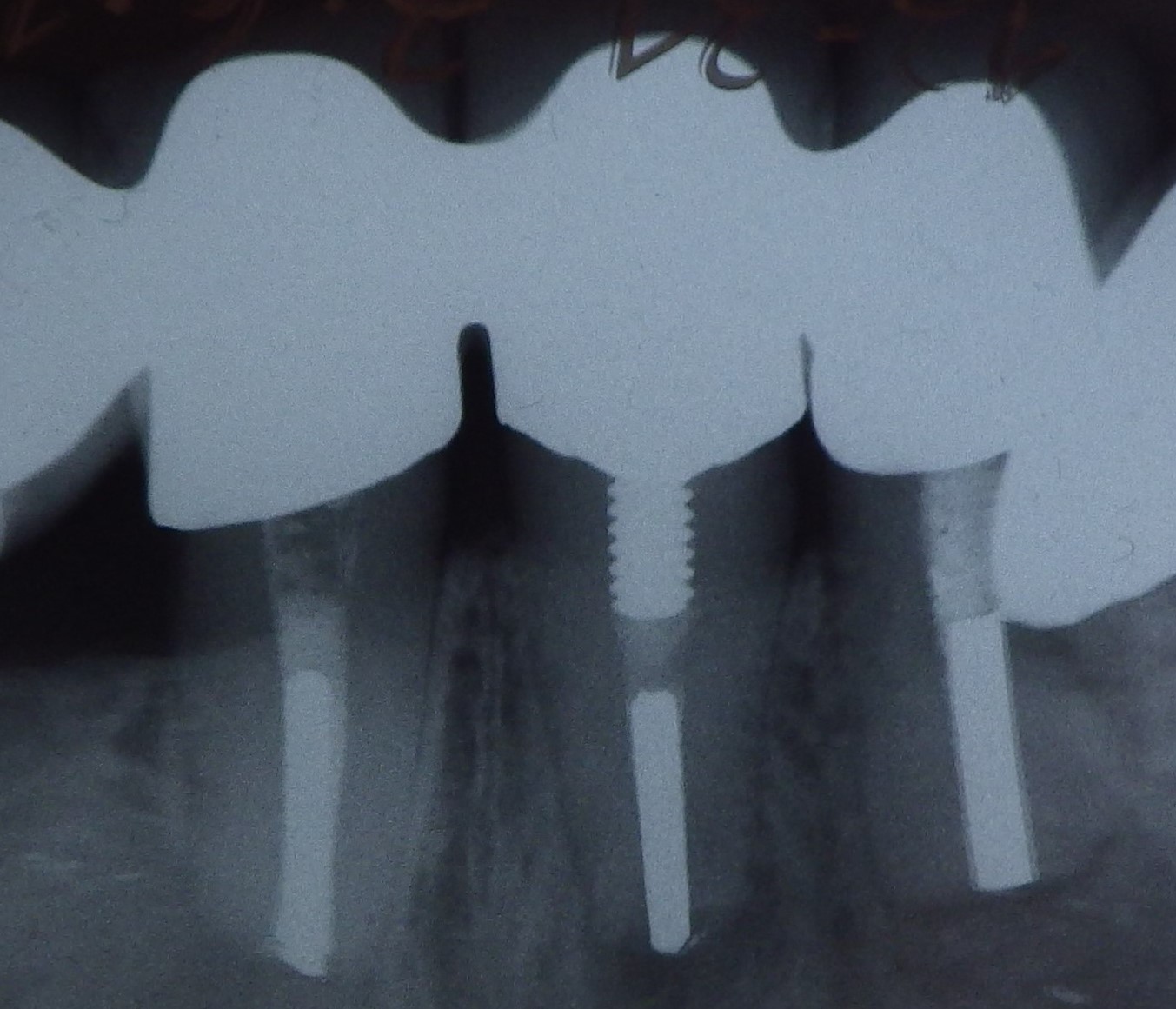 Three different root canal posts
Three different root canal posts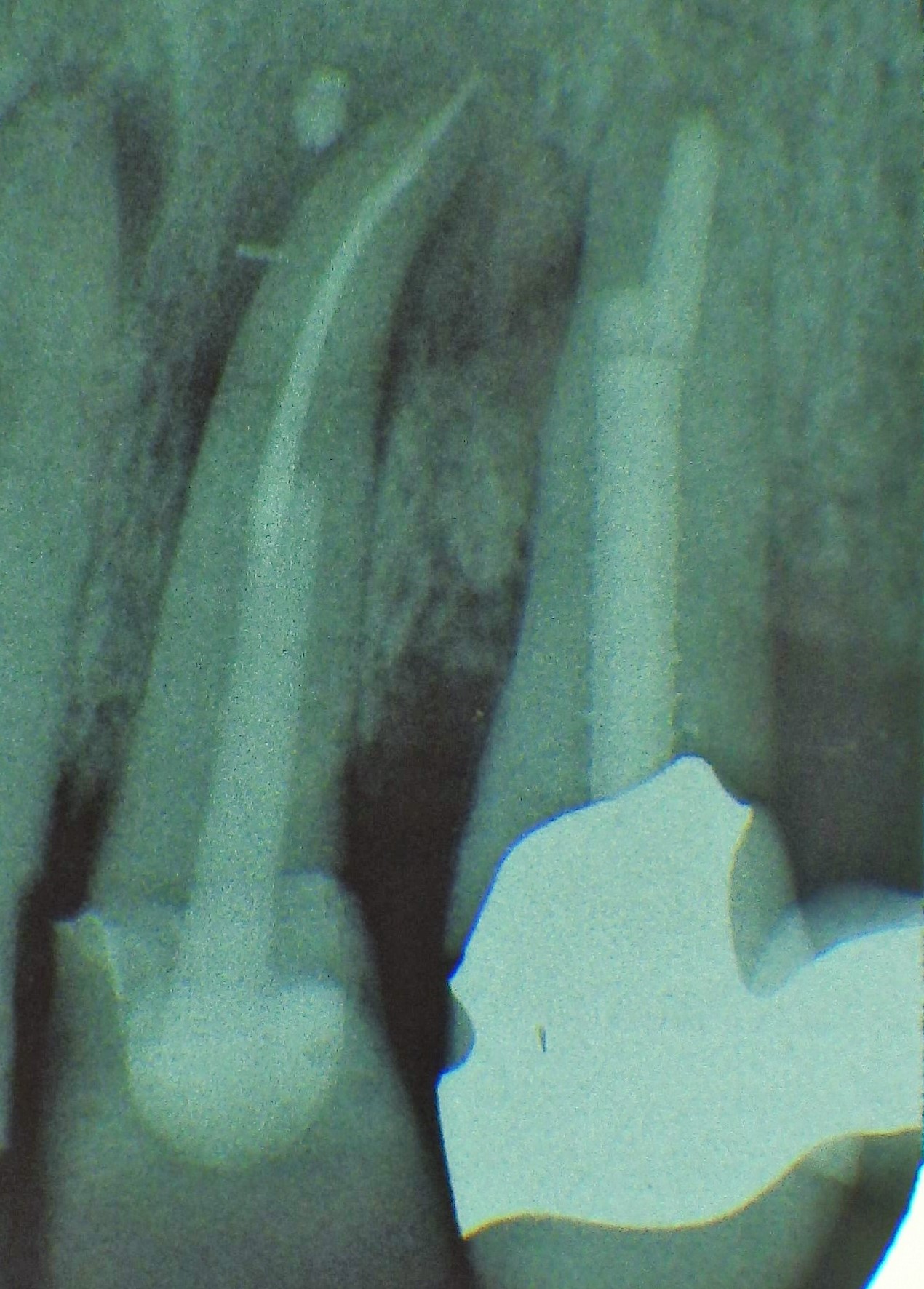 Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Tooth 14 conical and smooth, tooth 13 cylindrical and threaded