Orthodontics
Orthodontics
Indication and objective of orthodontic treatment
Orthodontics targets the desired alignment of teeth, dental arches and jaws in relation to one another and other anatomical structures according to aesthetic and functional concepts. All types of dysgnathia can be corrected, these include malocclusion of individual teeth (rotation, tipping, retention, elongation, malposition), malalignment of teeth in the dental arch (overcrowding, overlapping, diastemas), but also incorrect positioning of the maxilla and mandible to one another (occlusal anomalies).
Prophylaxis
Thumb-sucking and other habits are controlled or stopped and (also in interdisciplinary collaboration with other specialist disciplines such as logopaedics) swallowing or speech techniques are trained for example as prevention against malocclusion. Deciduous teeth should be preserved, if possible, or the spaces kept open (space maintainer) after loss of the deciduous teeth. Conversely, prophylactic extraction of teeth can also be practical.
Planning and documentation
In addition to clinical examination of the patient, mainly dental models and X-rays (orthopantomogram, OPM, OPG and lateral cephalometric radiograph LCR) are used in orthodontics for treatment planning and documentation of progress. Measurement in relation to reference points and lines are especially important for assessment.
Timing and duration of orthodontic treatment
In case of congenital anomalies, for example a lip-jaw-palate cleft, orthodontic treatment begins immediately after birth. With certain, highly pronounced and/or prognostically unfavourable malpositions early orthodontic treatments are indicated from age six onwards after eruption of the permanent incisors and first molars. The majority of treatments are performed during the juvenile growth phase before maximum puberty in the late mixed dentition between age nine and twelve. Corrections are also possible, however, with adult patients at any age, providing an alternative to other forms of dental treatments (e.g. dental restorations). The duration of treatment is measured in a minimum of months but generally a number of years may be required. To achieve planned treatment outcomes and prevent relapses retainers are fitted up to age 25 or 30 and sometimes also lifelong.
Forces and anchorage
Teeth are moved selectively by different types of biomechechanical forces (rotation, translation), which may be of natural (growth, movements, particularly in functional orthodontics, FO) or artificial origin. Mechanical appliances are often used as artificial sources of forces, e.g. resilient wires, compression and tension springs, elastics, expansion screws or plastic foils. In the balance between force and opposing force (actio = reactio) anchorage is always required, the stability of which must either be sufficiently predominant to remain practically unchanged or predictably moved in the opposite direction to the object of the movement. Other teeth or other groups of teeth can be used as anchorage as can alveolar bone or mini-implants inserted in the bone, as well as segments of the bony cranium (chin, forehead, back of the head). Forces in orthodontics must always be measured, so as to effect the required movement of teeth but without causing undesired side effects (e.g. resorption of the root cementum).
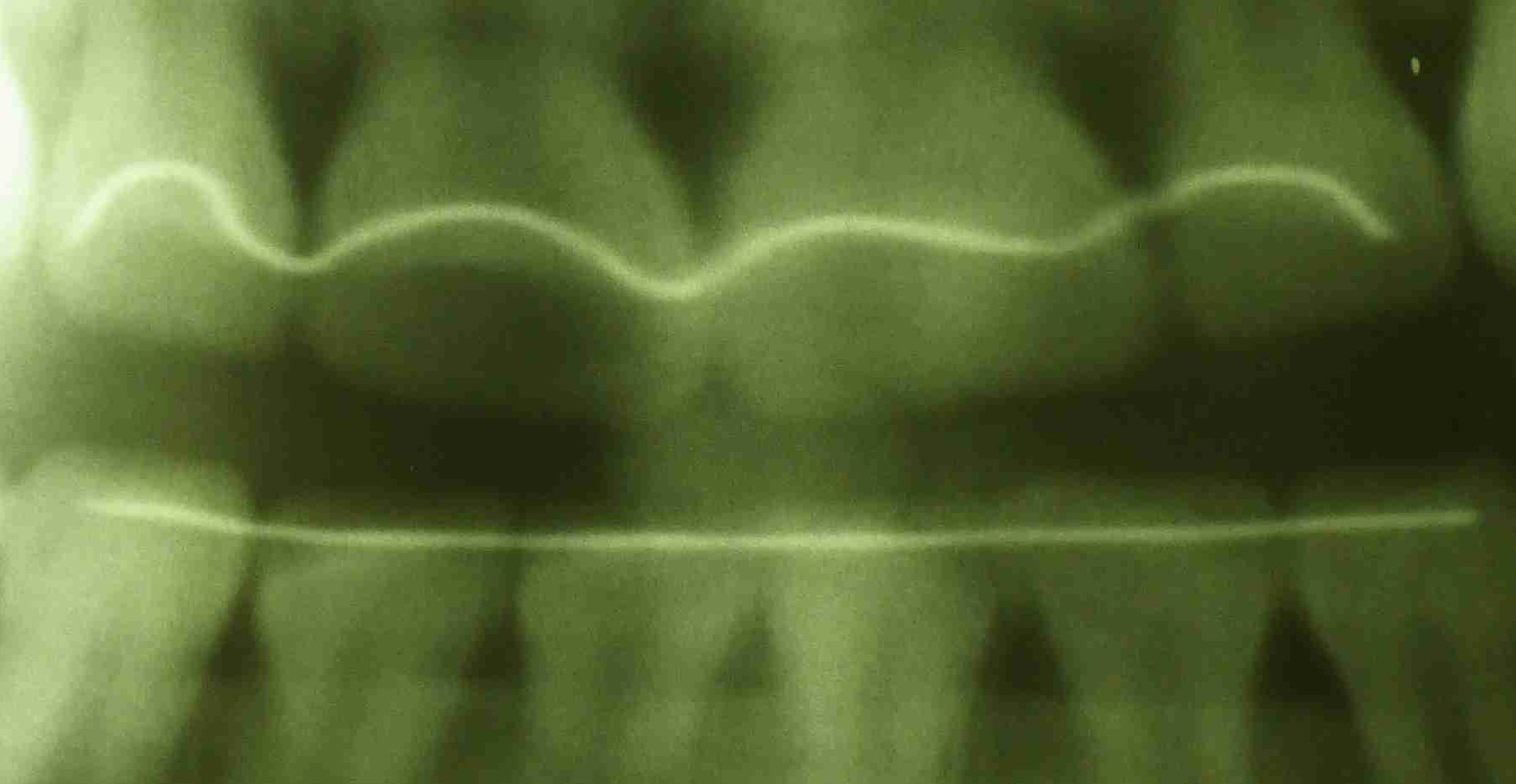 Upper and lower retentive bows (OPG)
Upper and lower retentive bows (OPG)
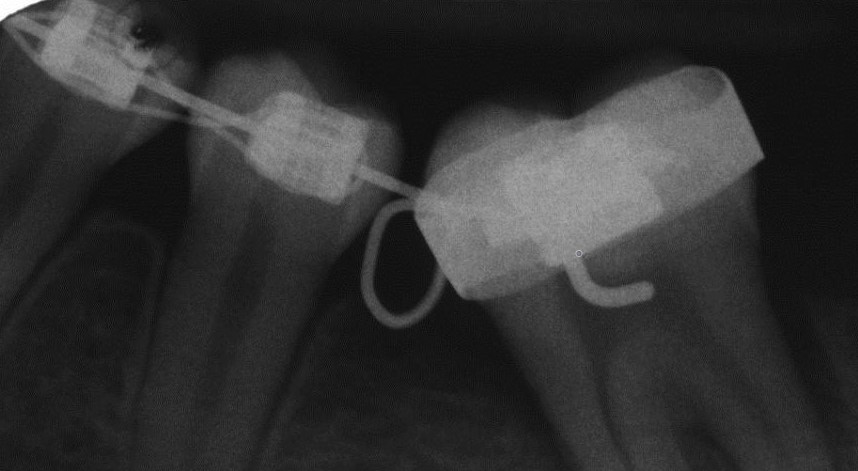 Brackets, molar band, ligatures (X-ray)
Brackets, molar band, ligatures (X-ray)
Appliances
Both fixed (e.g. brackets, bands, attachments, archwires) and removable appliances (e.g. activators and plates) are used in orthodontics. A differentiation is also made between extraoral (e.g. orthodontic facebows) and intraoral appliances. The latter can involve one or both jaws (bimaxillary appliances). Aesthetic orthodontics uses appliances that are as inconspicuous as possible, e.g. tooth-coloured archwires and brackets, transparent foils or lingual technique.
 Ceramic bracket with hook (© 3M)
Ceramic bracket with hook (© 3M)
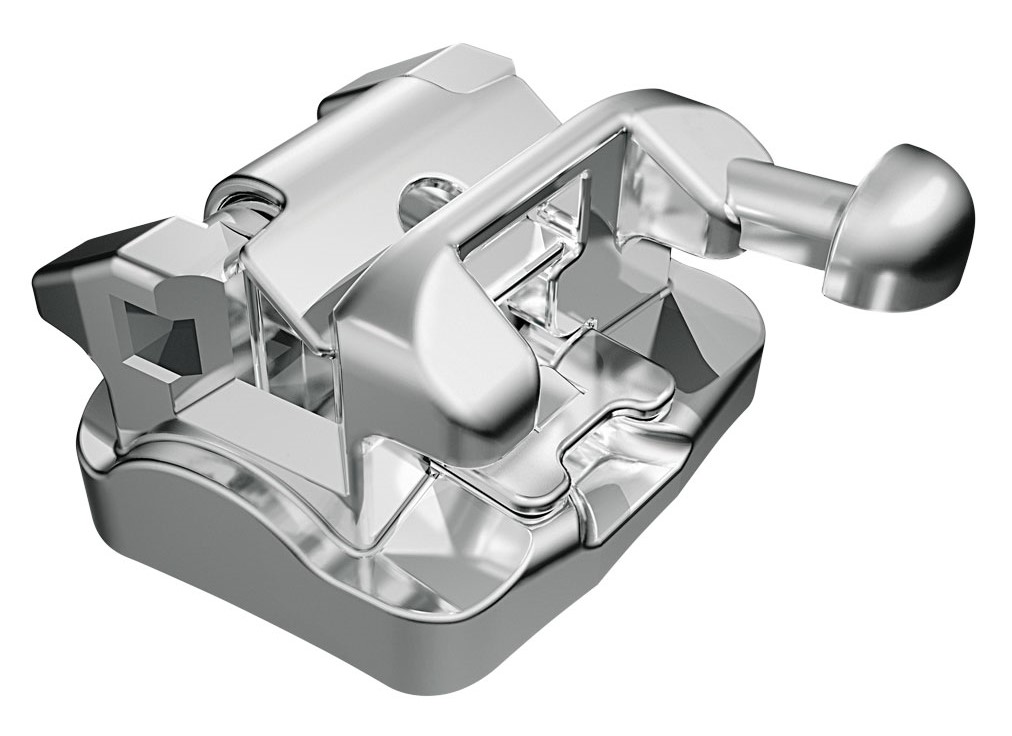 Self-ligating bracket (© FORESTADENT)
Self-ligating bracket (© FORESTADENT)
Surgery
Orthodontically indicated extraction of permanent teeth may also be required (extraction therapy) to remedy or prevent overcrowding. Serious malocclusions and anomalies of the jaw are also treated using orthodontic surgery, such as retention of permanent teeth using combined surgical-orthodontic procedures.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| non-keratinized | nichtkeratinisiert |
Focus text of the month
Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication… Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication for root canal posts. The preferred method is generally to insert the root canal post, so that it (by predrilling with ascending diameters) virtually fills the prepared post site and fits close to the dentine wall. That section of the root canal post in the root should be at least as long as the crown restoration, leaving a few millimetres of the root canal filling to seal the apex. Isolated concepts have also been developed with smooth metal posts projecting apically beyond the tooth and intended for anchoring in the bone (transdental fixation).
Restoration with a temporary post is seldom practical due to the increased fracture and reinfection rate; a definitive root canal post should be inserted as early as possible.
Customised root canal posts (often made from precious metal alloys), cast after waxing up directly in the root canal or indirectly after taking an impression of the root canal lumen (using burnout posts), can also be used for filling lumina with oval or irregular cross sections, as well as two or three divergent canals each fitted with a post inserted, if necessary, through the opening of another canal. The core build-up(s), or even the entire crown (historically: post crown) can be integrated. |
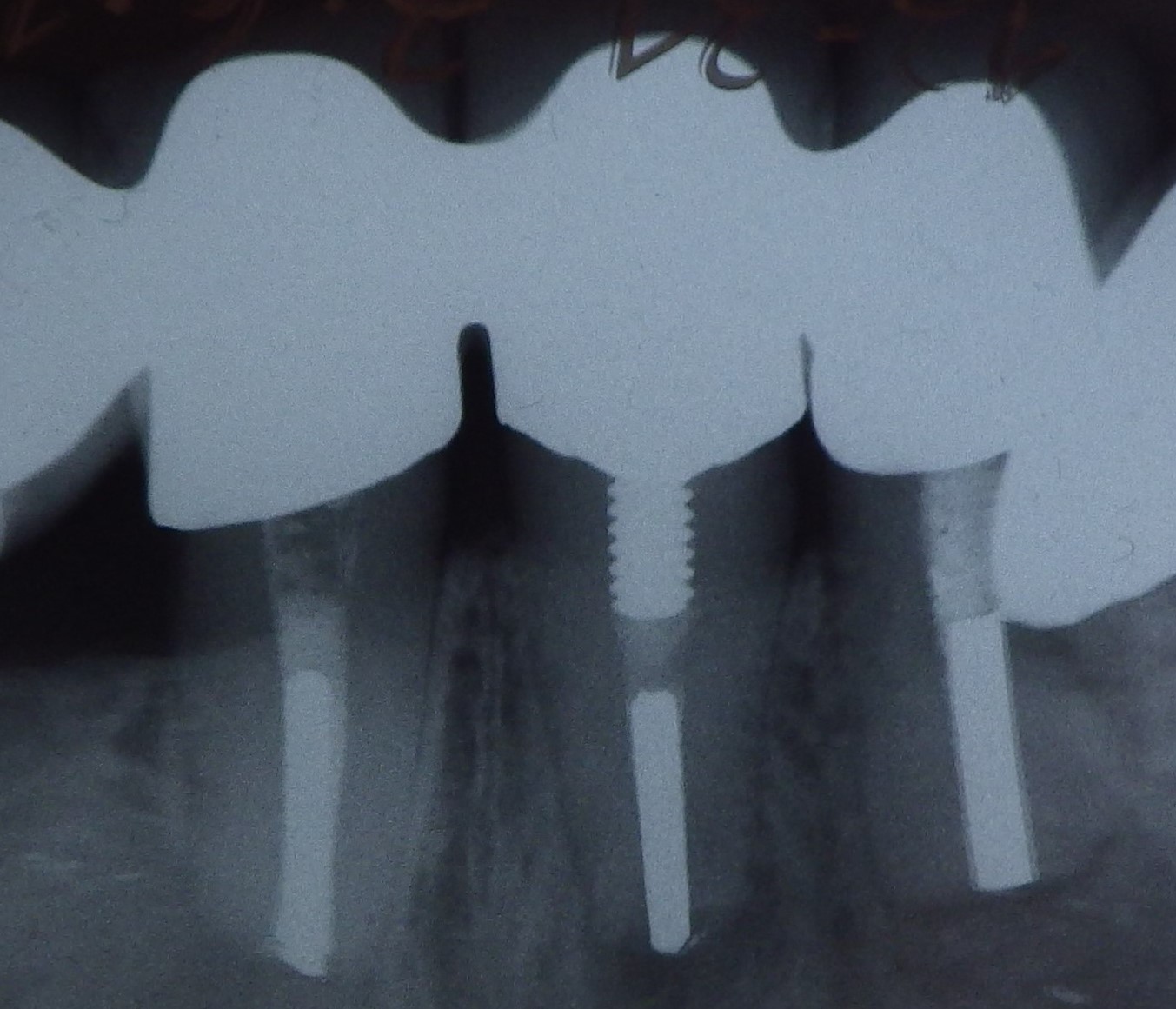 Three different root canal posts
Three different root canal posts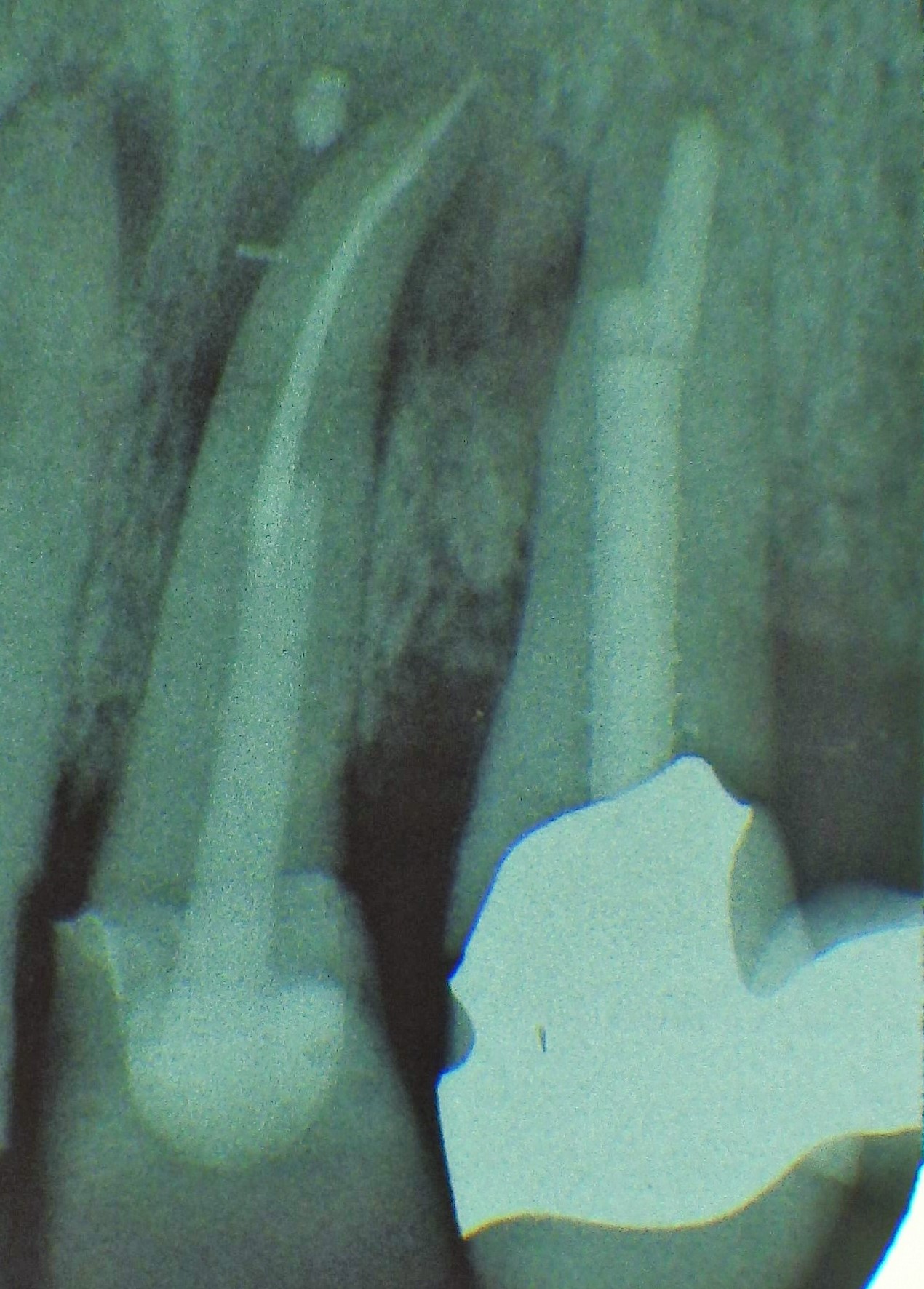 Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Tooth 14 conical and smooth, tooth 13 cylindrical and threaded