X-rays
X-rays
The invisible roentgen rays named after Wilhelm Conrad Röntgen (German physicist, 1st physics Nobel prize 1901 (initially referred to as "X-rays" in German, still called X-rays today in English]) are used for therapeutic, but mainly for diagnostic purposes in medicine, dentistry, structure and material testing.
The electromagnetic (ionising, i.e. uncharged molecules dispersed in ions and electrons) roentgen rays have shorter wavelengths than visible light. They penetrate body tissue and are biologically harmful, e.g. carcinogenic, (cancer-causing), mutagenic (gene-changing) and teratogenic (embryo-damaging). This is why the frequency (i.e. the number of X-ray images) and the respective single dose must be limited to the absolutely necessary in order to minimise radiation exposure. Areas that should not be irradiated must be shielded using suitable materials (mainly lead, e.g. in X-ray shields, radiography aprons, X-ray protective doors etc.).
Diffraction of X-rays allows conclusions to be made about the structure of molecules (DNA), crystals and materials. Emission of element-typical spectra of X-rays after irradiation with electrons or X-rays (X-ray fluorescence) enables analysis of the chemical elements contained in the substances.
Orthopaedic pain levels ("X-ray inflammation irradiation") and tumour cells, which are sensitive to radiation, can be combated using X-rays. The (e.g. intraoperative) X-raying of body structures (using radiographic image intensifiers) is used for analysis of processes and optimisation (e.g. reposition of fractures).
Occasions for using diagnostic X-rays can be acute complaints, traumata or disease status, but also exclusion and early diagnosis of damage (bitewing X-ray for early detection of caries) as well as planning and follow-up of dental treatment measures (surgery, endodontology, implantology, orthodontics, prosthetics).
 Extensive carious cavity in tooth 27
Extensive carious cavity in tooth 27
 X-ray image
X-ray image
In dentistry intraoral X-ray tubes (X-ray sources) are rarely used, though extraoral X-ray tubes are mainly used to irradiate analogue, light-sensitive X-ray films (chemical development and fixation in the darkroom), X-ray imaging plates (stimulation of fluorescent substance, scanning using lasers) or digital X-ray sensors (CCD or CMOS semiconductor devices). The X-ray voltage of "conventionally" used X-rays is 60 to 70 kilovolts. Two-dimensional images are created using static systems (dental film, lateral cephalometric radiograph, temporomandibular images) and orthopantomograms and three-dimensional images (CT = computer tomography, CBCT = cone-beam computed tomography) are created using rotary systems. The images are viewed on X-ray viewers (analogue) or (if necessary, combined with image processing) on the computer monitor (digital).
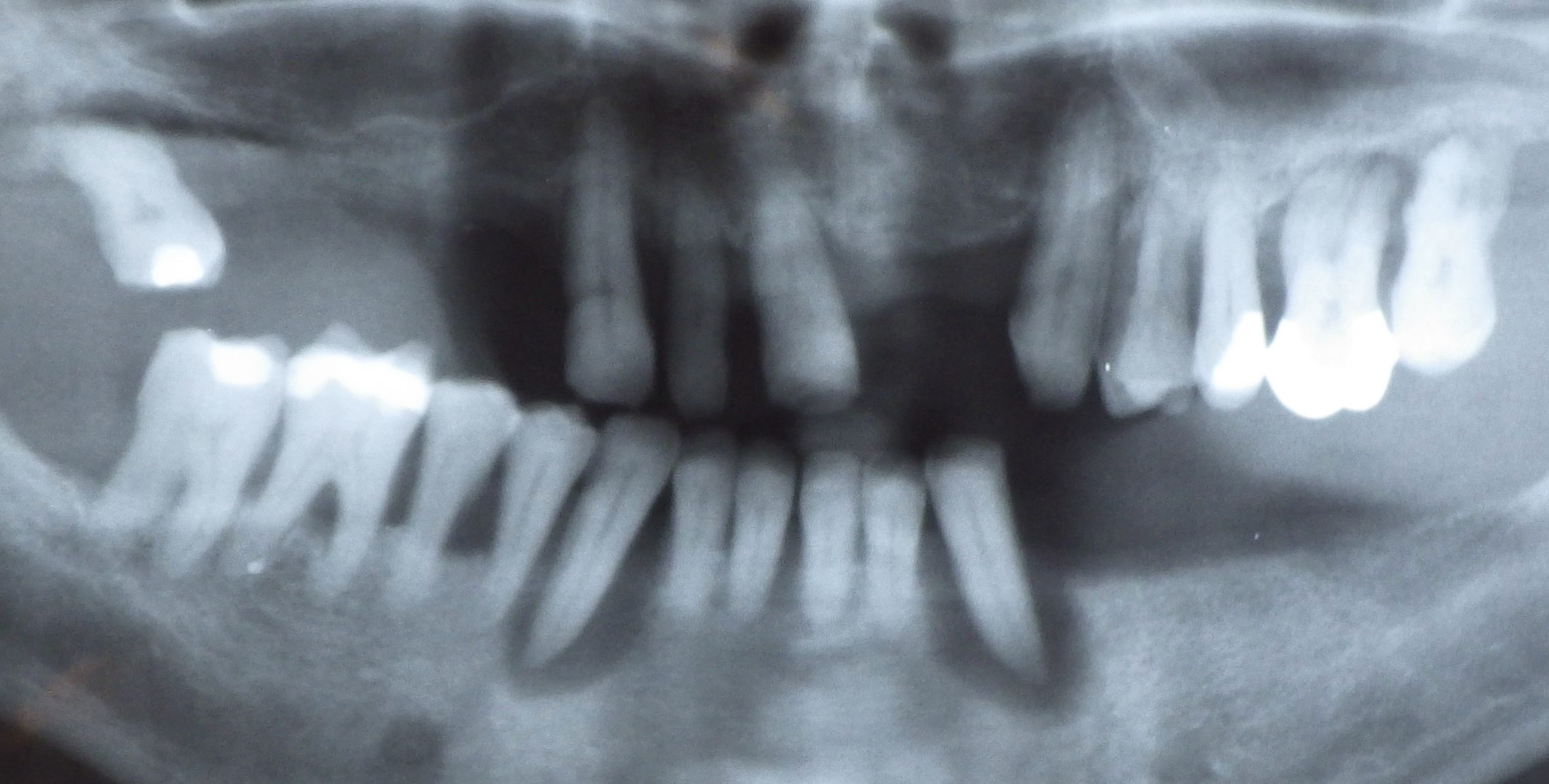 Panoramic X-ray, orthopantogram
Panoramic X-ray, orthopantogram
.jpg) Orthopantogram of an 8-year-old (deciduous dentition)
Orthopantogram of an 8-year-old (deciduous dentition)
Different body tissues contain varying amounts of chemical elements whose proton count in the atom nucleus differ and consequently their absorption of the X-rays, which shows as image contrast, e.g. between hard structure with a different calcium content (bone, dentine, dental enamel) and soft tissue. A greyscale image is created with a resolution of up to 20 line pairs per millimetre or 25 µm. The usual negative representation leads to correspondingly "reverse" terminology, lighter areas are defined as shadowing and darker areas as brightening.
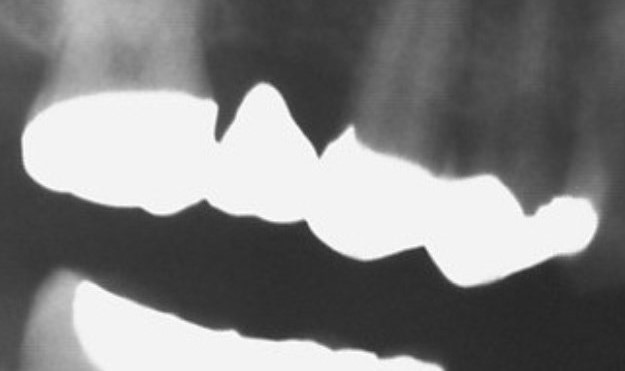 Bridgework spanning teeth 15 - 17
Bridgework spanning teeth 15 - 17
Metal foreign bodies (amalgam, cast restorations) and ceramics placed in the oral cavity normally have a high degree of radiopacity and appear white or light grey. Filling materials (temporary sealers, composite and gutta percha) medication (calcium hydroxide paste) or acrylics and denture teeth for X-ray templates can be made radiopaque using positive X-ray contrast materials.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| burning mouth syndrome | Mundbrennensyndrom |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration