Fixed restorations
Fixed restorations are a part of prosthetics. In particular crowns (though they often do not replace a tooth but only supplement the lost tooth structure of an existing tooth) and bridges as well as bar restorations are described as fixed restorations. Implants replace "fixed" tooth roots in the bone but are not defined as fixed restorations.
In contrast to removable restorations, fixed restorations are rigidly bonded to teeth or implant abutments using adhesive retention or cementation. Restorations, which are fixed for the patient (e.g. by screw-retention or temporary cementation) but are designed to be removable by the dentist, are called "operator-removable". If restorations, which are removable for the patient, are retained on fixed crowns they are called fixed-removable restorations.
A minimum of four periodontally healthy abutments in a favourable alignment (quadrangular) is essential for ensuring stable, statically balanced support per jaw for purely fixed restorations. However, for purely implant-borne fixed restorations in particular, a minimum of six abutments is required in the mandible and even eight abutments in the maxilla due to the lower bone quality. An increase in the number of abutments (e.g. using implants) and also a combination using removable (tissue-borne) restorations can help relieve the natural residual teeth.
 Pontic 42, labial view of single-winged bridge
Pontic 42, labial view of single-winged bridge
 Pontic 42, clinical view of single-winged bridge
Pontic 42, clinical view of single-winged bridge
Features of fixed restorations are periodontal support on abutments, a rigid, immovable connection with the abutment and the subjective sensation of patients of wearing "their own teeth". Care and repair are more difficult compared with removable versions and extending the restoration is generally impossible – especially in the case of (primary) connections with adjacent single crowns for increasing the stability. This is why the previously generally accepted superiority of fixed restorations should be qualified according to each individual case.
A fixed restoration is not only impossible in edentulous cases but also with implants if, as a result of massive bone resorption, the distance between the alveolar ridge level and occlusal plane is too large, which would lead to an excessively forceful leverage effect.
Fixed restorations can be fabricated provisionally (temporary; generally using acrylic and rarely from metal or ceramic), e.g. for testing a new occlusal relationship or for bridging the time required for fabrication of the permanent restoration or other treatment.
Individual components of fixed restorations can be prefabricated (e.g. attachments, other connectors or implant abutments); these can remain unchanged or they can be customised. Final (permanent) fixed restorations are fabricated either from a single material, combinations of materials or by joining different materials using very different procedures, e.g. casting, milling, soldering, welding, grinding, sintering (CAD-CAM), pressing or electroforming.
Temporary luting (short, medium or long-term) can be used for trying in fixed restorations.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| polishing debris | Polierreste |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms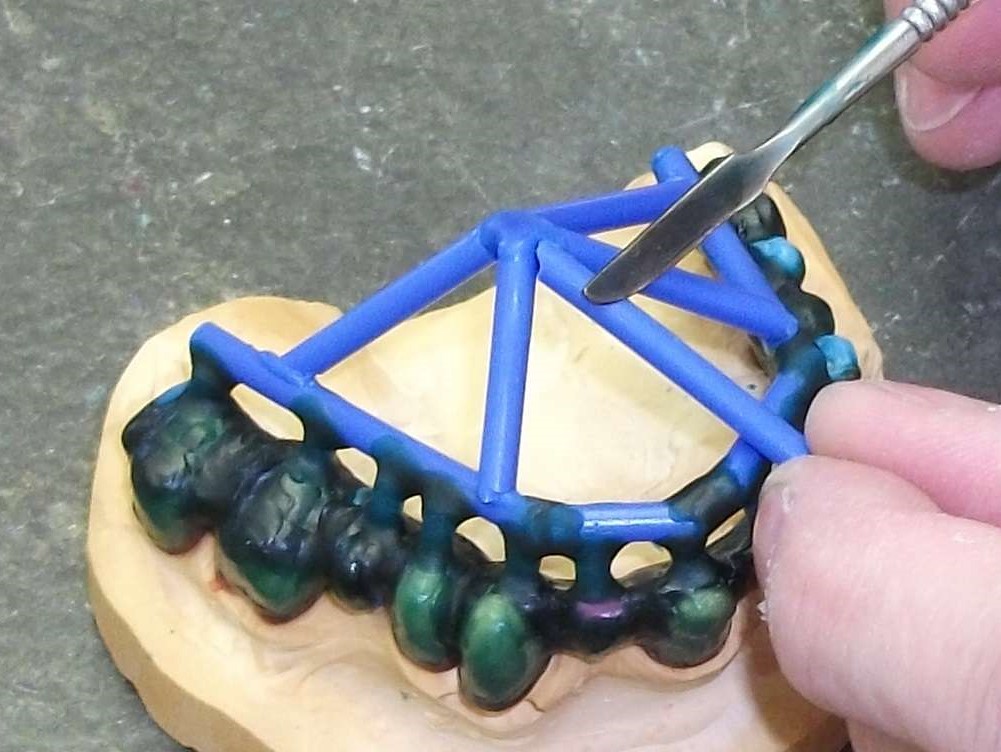 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument