CMD
CMD (craniomandibular dysfunction) is a collective term for different types of disorders of the normal function of the masticatory organ (also called "masticatory apparatus", comprising teeth, jaws, tongue, temporomandibular joints, masticatory musculature, neural circuits involved and adjacent anatomical structures) with multiple symptoms. Alternative terms are craniovertebral dysfunction (CVD), myoarthropathy, stomatognathic dysfunction, temporomandibular dysfunction (TMD) etc.
The symptoms of CMD can be roughly divided into the areas of joint problems (arthropathy), displacement of the disc (discopathy), myofacial pain (myopathy) and other physical and psychological symptoms. In particular in the temporomandibular joint it can lead to pain, cracking or rubbing noises, restriction of the mouth opening or even to lockjaw. There may be lateral deflection, deviation from the straight, vertical mouth opening. Increased mobility of the mandible is also possible; the mandible can also dislocate (lockjaw, luxation), e.g. with a wide yawn. Frequently tension and pain may occur in the regions of the masticatory musculature, head, face and neck. In rare cases earache, ringing in the ears (tinnitus), dry mouth or taste disorders can also occur.
In addition to a general dental examination and diagnosis, first an orientating test (rapid test) is required in cases with indications for CMD followed by comprehensive diagnosis of the masticatory system (functional analysis, functional diagnostics) for detection and more precise determination of CMD. This includes manual examination of temporomandibular joints and musculature (manual functional analysis), with special measuring devices (instrumental functional analysis) and often also special X-rays (temporomandibular joint X-ray) as well as standardised questionnaires for collecting specific patient case histories. Findings are recorded and evaluated in a standardised form (functional status).
Apart from general illnesses (rheumatics, arthritis, muscle and nerve diseases), possible causes of CMD are congenital and acquired tooth malalignment (tipping, rotation, extension), intercuspation and occlusal relationship disorders ("occlusopathy", cross-bite, edge-to-edge bite, deep overbite, open bite), diastemas, incorrect vertical relationship of dentures, bridges, crowns or fillings, misalignment of the locomotor system, accidents, overloading and overstretching (power sports, intensive chewing of gum, long-term tooth treatments, operations under general anaesthetic, parafunctions (habits) such as biting nails/pencils and bruxism (clenching, grinding) and also stress and mental/psychological strains and disorders (psychosis, depression, anxiety disorders). There is seldom only one single cause; mainly several factors are collectively involved in the development of CMD (multifactorial aetiology).
Many dysfunctions are low grade and harmless. Serious dysfunctions can also be pain-free (referred to as "compensated CMD") or accompanied by passages of pain to frequent and/or long-lasting pain. Long-term dysfunction can result in damage to parts of the masticatory apparatus, in particular to teeth (heavy attrition), periodontium (periodontitides) and temporomandibular joints (attrition, habitual luxation) and also to persistent neuropathies ("trigeminal neuralgia"). Clearly identifiable, disturbing or painful CMD should therefore be treated.
Mutual interaction between CMD in the cranial region, changes in posture and other further-removed sections of the locomotive system, (musculoskeletal system), e.g. head, neck, shoulders, vertebral column, hips, knee and feet) as well as psychological factors often render interdisciplinary collaboration therapeutically practical, for instance between the dentist, orthopaedist, physiotherapist, psychotherapist etc.
Initially, easily reversible and/or less invasive (minimally invasive) treatment options are selected, such as short-term pain relief (using analgesics, cold or warm application), prevention and self-help (light food, movement and relaxation exercises), physical and physiotherapy, psychosomatic medicine and also removable splints. Different types of laboratory-fabricated splints are regularly used during treatment of CMD. The objectives of splint therapy include: reversing and re-orientation of the masticatory system, relaxation of the musculature; changing the position of the condylar head (retraction, reposition, distraction; protection of teeth and restorations against attrition, cracks, breaking off and protection of the periodontium against overloading.
Irreversible (invasive) treatment approaches (e.g. heavy systematic grinding-in, restoration, orthodontics, operations) are mainly reserved for serious courses of diseases.
CMD and other areas of dentistry are closely interrelated: CMD should be excluded or treated (to ensure success) before undertaking extensive (conservative or prosthetic) restorations, if necessary these will also be fitted to safeguard a new pain-free "therapeutic" occlusal relationship acquired during CMD treatment. Orthodontic treatment is intended to avoid favourable conditions for CMD, though it can also be used for its treatment. Conversely, CMD therapies can display orthodontic effects.
All aspects of CMD have been the subject of intensive technical dispute for decades between sometimes mutually exclusive approaches. In addition to terminology, aetiology, diagnostics, manifestation and meaning of CMD, all treatment approaches (whose evidence-base encounters systematic difficulties) are fundamentally called into question time and again.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| feeding aid | Fütterungshilfe |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms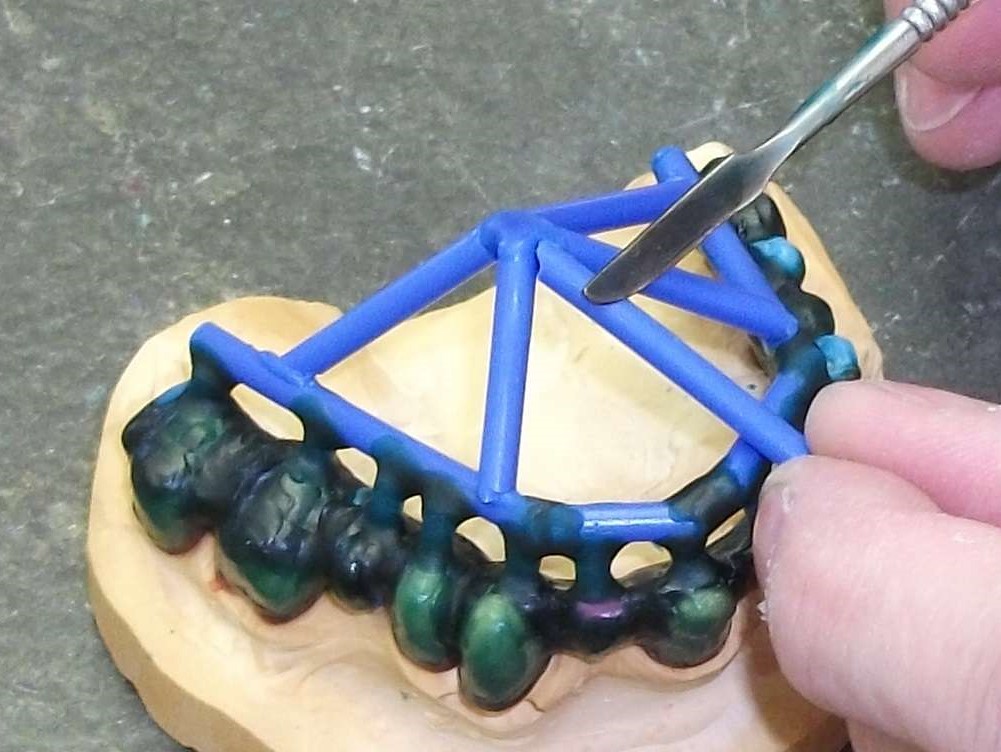 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument