Endodontics
Endodontics
Types of treatment, which affect the interior of the tooth and the area around the root tip, are collectively termed endodontics (endodontic treatment).
Endodontologists are dentists specialised in endodontics. Endodontics is a section of conservative dentistry and therefore always supports tooth conservation. This includes (direct) pulp capping of exposed pulp area, apicectomies but mainly root canal treatment. Endodontic treatment is indicated with irreversible pulpitis, destruction of the pulp due to accidents or infection as well as persistent or re-occurring bacterial colonisation of root canals that have already been treated or filled (revision).
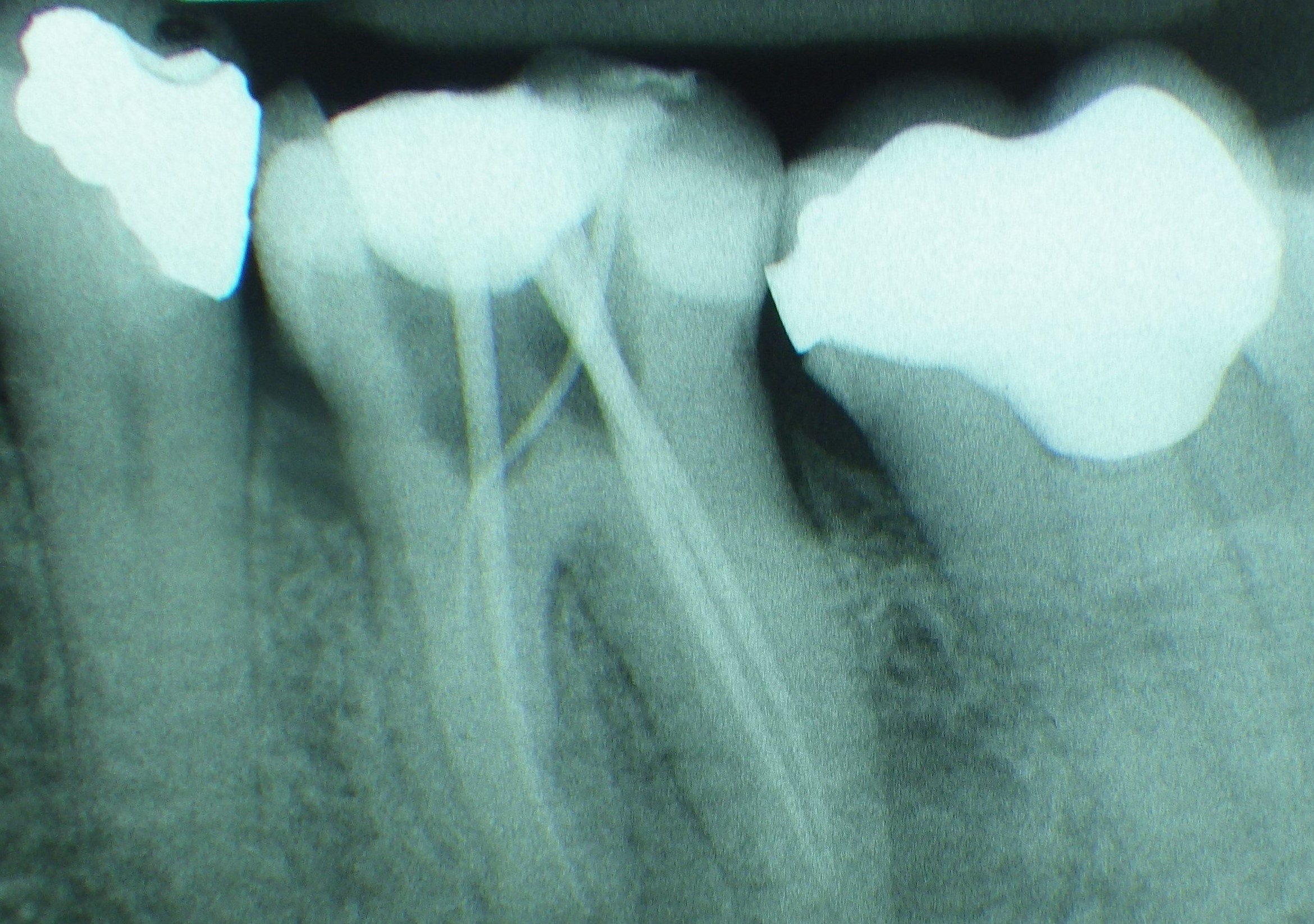
 Access to the pulp chamber
Access to the pulp chamber
The initial aim (practical) is the complete elimination of diseased tissue, foreign material (e.g. existing root canal filler material) and pathogens from the root canal system. The chemical methods include antibacterial and/or tissue-dissolving solutions (e.g. chlorhexidine, EDTA, sodium hypochlorite, hydrogen peroxide). Machine or manually operated steel or nickel titanium root canal instruments are used for mechanical preparation, i.e. excavation, smoothing, cleaning and extension of the (main) root canals. Both methods in combination form chemomechanical preparation. Medical temporary fillings (e.g. with calcium hydroxide or chlorophenol camphor menthol) can be used for further reduction of bacteria. Finally, the prepared main root canals are obturated, i.e. using a root canal filling (e.g. consisting of gutta percha posts and root canal cement) filled, sealed and covered using an adhesive filling and/or a crown.
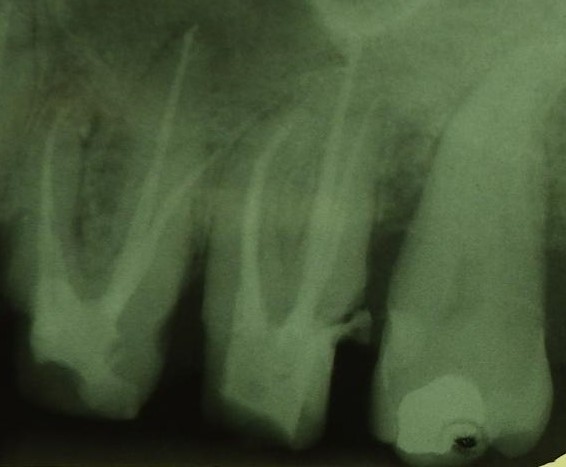 Filled root canals 25, 26, 27
Filled root canals 25, 26, 27
 Master point - The first guttapercha point
Master point - The first guttapercha point
In the final outcome the treated tooth should heal long term without any discomfort/symptoms and there should be no pathological changes of the apical alveolar bone (detectable on the X-ray). The probability of success of endodontic treatment has greatly increased in the past two decades, particularly due to the increased use of operating microscopes and microsurgical techniques and is generally given as 90%. In addition, successes have been achieved in the coverage (including iatrogenic) of perforations or the removal of fractured instruments or cemented posts from the root canal system.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| feeding aid | Fütterungshilfe |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms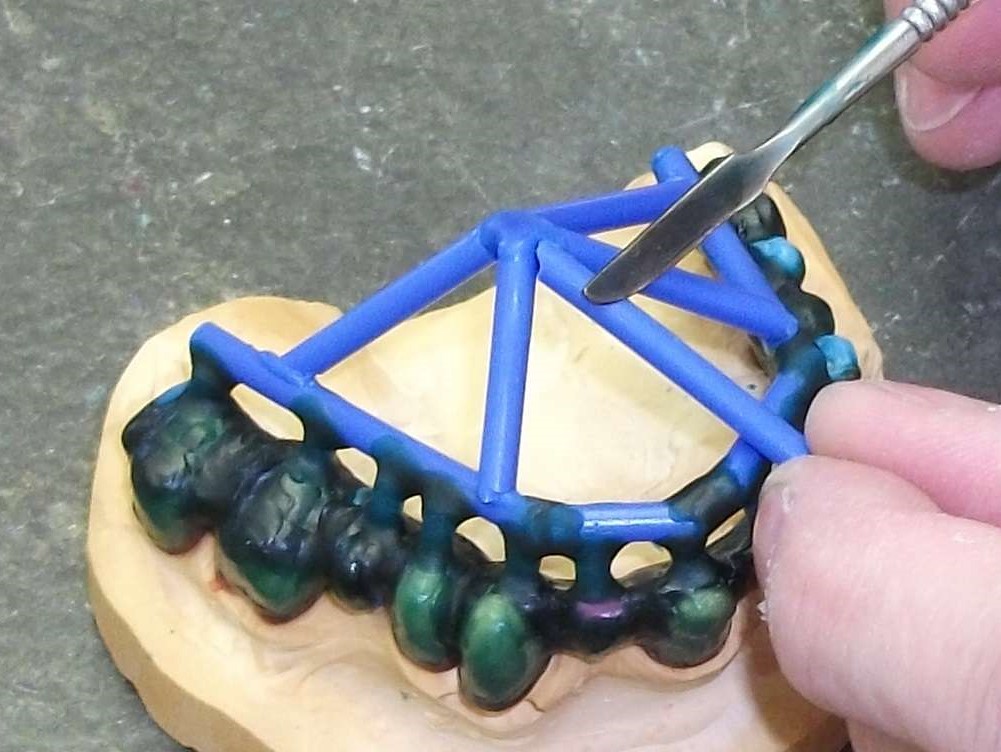 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument