Root canal post
Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication for root canal posts. The preferred method is generally to insert the root canal post, so that it (by predrilling with ascending diameters) virtually fills the prepared post site and fits close to the dentine wall. That section of the root canal post in the root should be at least as long as the crown restoration, leaving a few millimetres of the root canal filling to seal the apex. Isolated concepts have also been developed with smooth metal posts projecting apically beyond the tooth and intended for anchoring in the bone (transdental fixation).
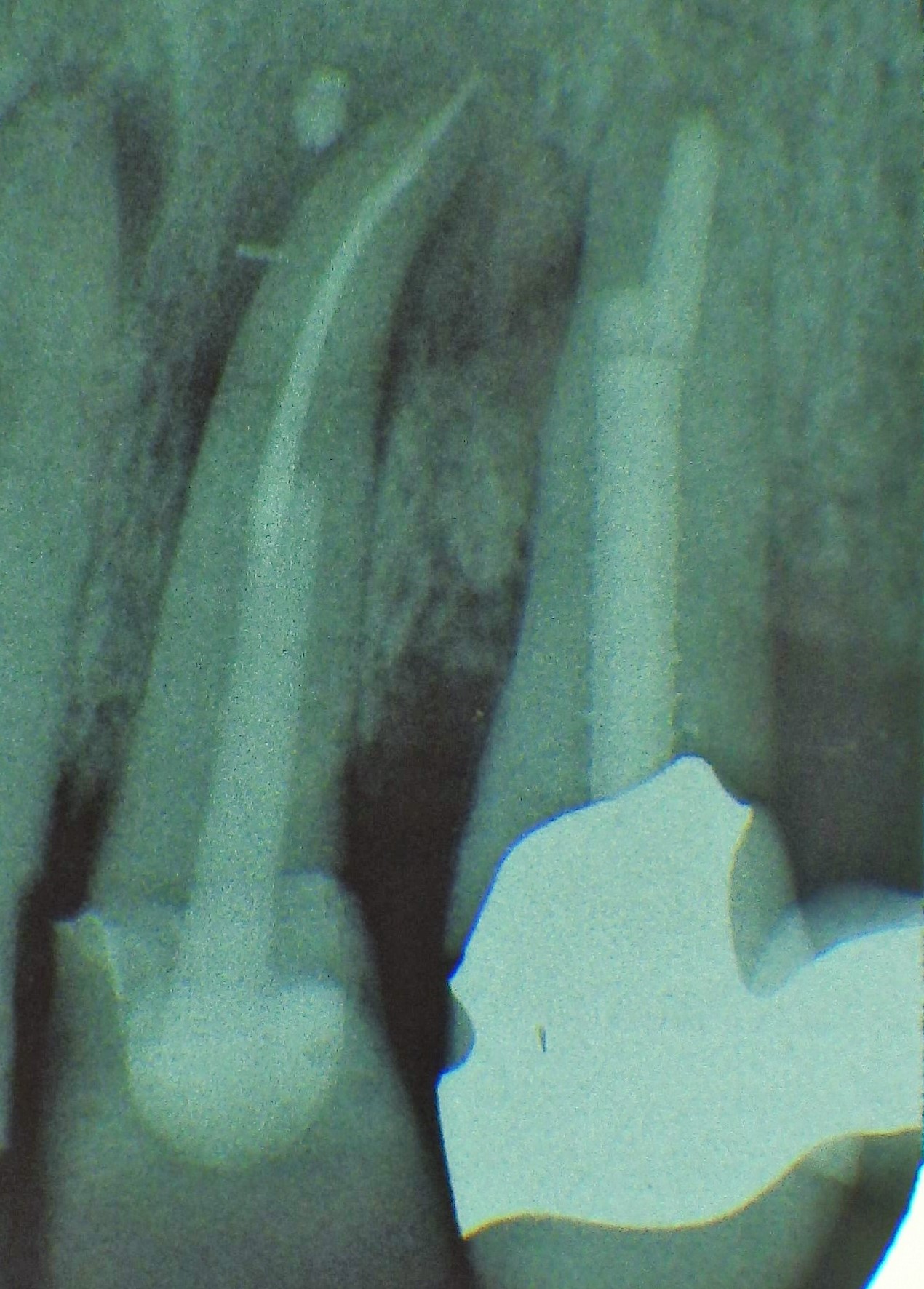
 Three different root canal posts
Three different root canal posts
Restoration with a temporary post is seldom practical due to the increased fracture and reinfection rate; a definitive root canal post should be inserted as early as possible.
Conventional conical (root-shaped) or cylindrical root canal posts are mainly made from metal alloys. Prefabricated root canal posts, e.g. manufactured from steel or titanium are rarely smooth, but often have a screw thread to provide anchorage in the dentine and escape channels for conventional luting cement as well as a retentive head for building up a core. In addition to rigid root canal posts, flexible posts are available for adapting to the coronal anatomy.
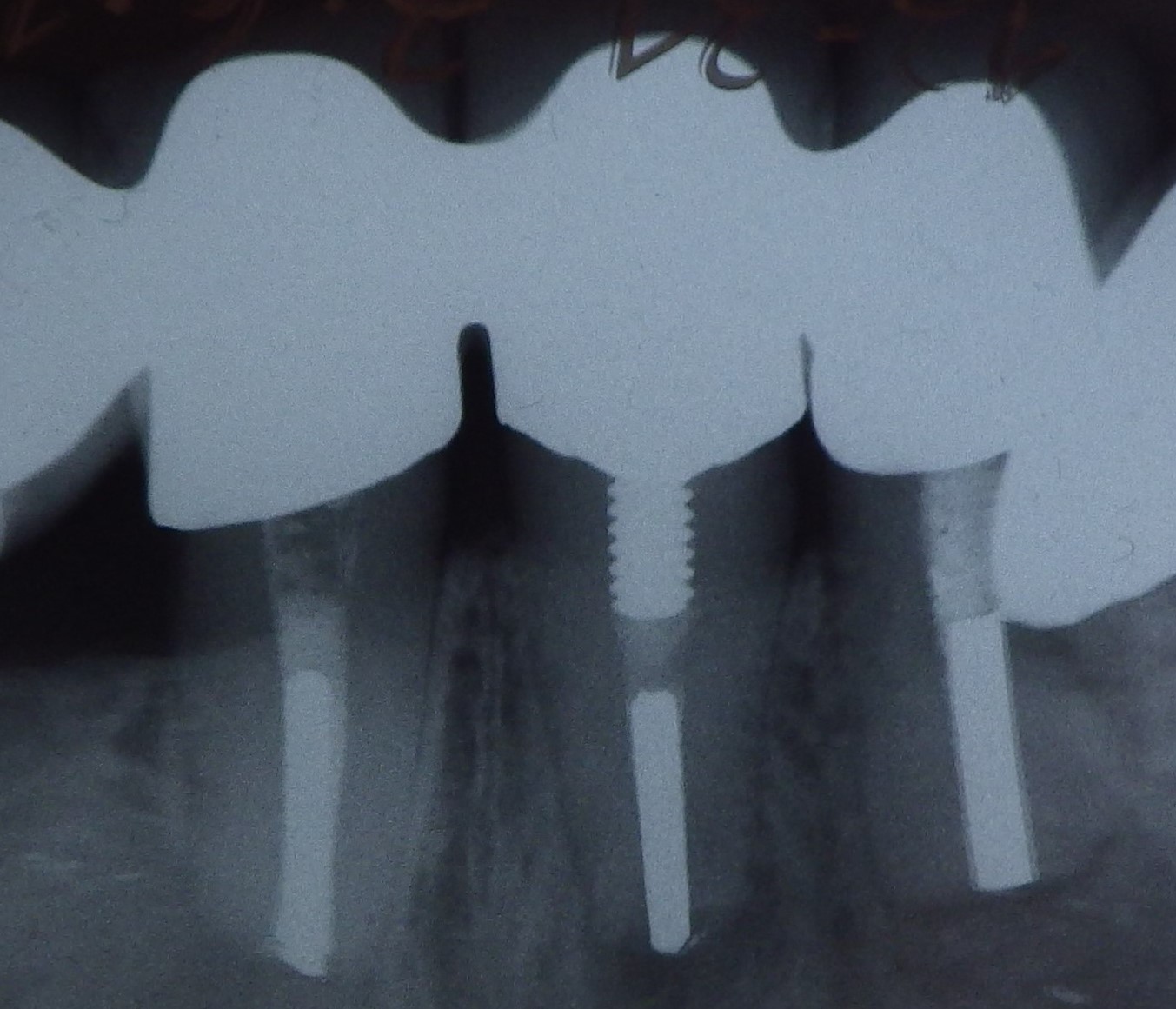
 Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Customised root canal posts (often made from precious metal alloys), cast after waxing up directly in the root canal or indirectly after taking an impression of the root canal lumen (using burnout posts), can also be used for filling lumina with oval or irregular cross sections, as well as two or three divergent canals each fitted with a post inserted, if necessary, through the opening of another canal. The core build-up(s), or even the entire crown (historically: post crown) can be integrated.
Up to about the end of the 20th Century root canal posts (also called endodontic posts) were still regarded as a standard, stabilising reinforcement of a root-filled tooth, which would generally be crowned later. In the meantime, the tooth structure of devitalised teeth is known to be just as stable as that of vital teeth. Its increased fracture susceptibility is only caused by mechanical weakening due to loss of tooth structure; a root canal post therefore does not increase the strength.
Today, mainly conical (prevents excessive weakening of the remaining tooth wall apically) and smooth, rotationally symmetrical (in order not to build up any compressive or tensile stresses) root canal posts are inserted. These are often no longer manufactured from metal but mainly from glass-fibre resin composites and, more seldom, carbon fibre or zirconia. This makes them highly suitable for the predominant adhesive anchorage in root canals using silanization and, if possible, (due to problematic light access) chemical or dual-curing adhesives and luting composites. The main function of modern root canal posts is to enlarge the retentive surface for restorations also retained adhesively on the residual tooth structure (mainly with a circumferential retentive rim of approx. 2 mm vertically). The fibrous structure also provides a certain flexibility, which corresponds to that of dentine and therefore prevents cracking of the root created by coronal leverage forces on the one hand and loosening ("nail-pulling effect") on the other. These two phenomena were previously the main causes for failure of post restorations.
Glass-fibre posts can be removed relatively easily; the fibres function as guide rails for the respective rotary instruments.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| lip-sucking | Lippensaugen |
Focus text of the month
Wax build-up technique Wax build-up technique The various anatomical structures (such as cusp tips and slopes as well as marginal ridges) are usually built up one after another by adding small portions of wax (often using differently coloured waxes for didactic purposes). The firm, special waxes first have to be melted at room temperature. This can be carried out by warming small portions on differently shaped working tips of hand instruments in an open flame (such as a gas burner) or using electrically heated instruments which provide for more accurate temperature control and avoid contamination (e.g. electric wax-knife, induction heaters, wax dipping units). The wax is applied drop-by-drop to ensure that the warmer molten wax added last fuses seamlessly with the firm, cooler material. After hardening, the wax pattern can be reduced by sculpting, milling guidance surfaces or drilling to add retainers. Modern procedures include flexible, occlusal preforms for adding contours to soft wax. In addition, wax preforms, such as for occlusal surfaces or bridge pontics, are available in various shapes and sizes. Recently, irreversible, light-curing materials have been introduced for use instead of reversible thermoplastic waxes.
To ensure that the wax pattern can be released without being damaged, model surfaces, opposing dentition and preparations must be hardened/sealed with special lacquer (applied by spraying, brushing or dipping). These waxes are mostly relatively rigid/elastic after cooling.
When employing the lost wax technique, prefabricated wax sprues, bars and reservoirs are attached to the patterns. Once the pattern has been released and its sprues waxed onto the crucible former, it is invested in a casting ring with refractory investment material. The wax can then be burnt out residue-free and casting completed. Unlike standard wax build-up techniques, a diagnostic wax-up is not intended for fabricating an indirect restoration, but rather for simulating the appearance and/or external contouring for producing orientation templates. |
 Wax preforms
Wax preforms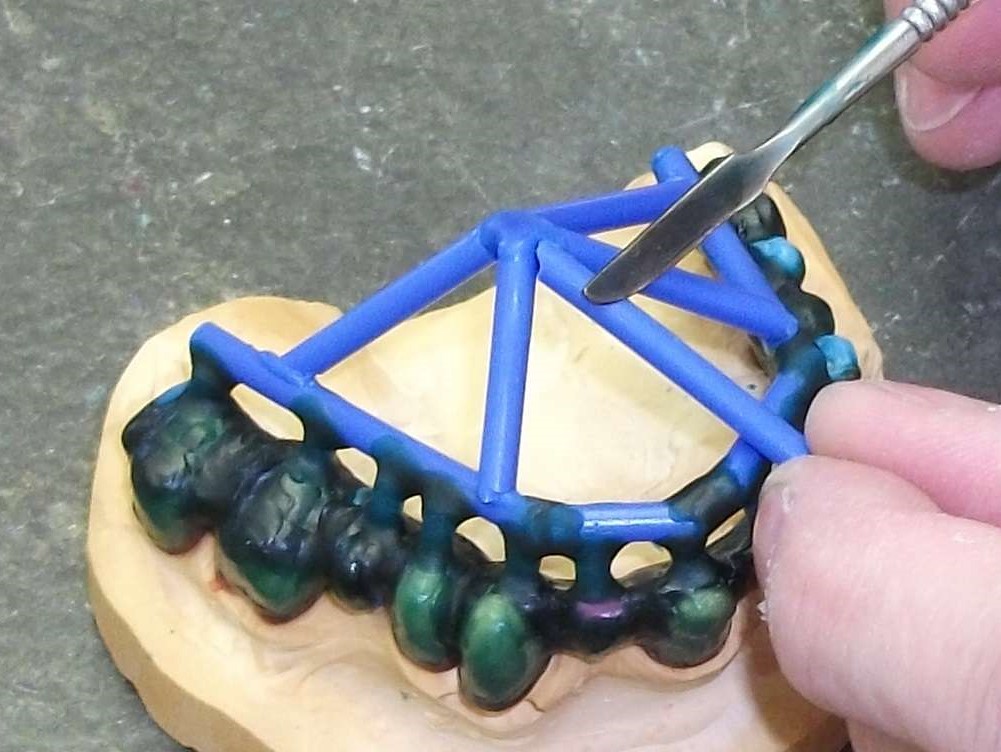 Attaching wax sprues to a removable framework supported on double crowns using a hand instrument
Attaching wax sprues to a removable framework supported on double crowns using a hand instrument