Strahlgeräte in der Zahntechnik
Strahlgeräte in der Zahntechnik
Das Bearbeiten von Werkstücken mittels Strahltechnik findet in entsprechenden Strahlgeräten statt.
In Feinstrahlgeräten dienen "Strahlgriffel" zur manuellen Bearbeitung einzelner Werkstücke. Daneben gibt es Umlaufstrahlgeräte, mit denen zusätzlich mit feststehenden (ausrichtbaren) Strahldüsen automatisch mehrere ähnliche Werkstücke (etwa Modellgussgerüste) in einem langsam rotierenden Strahlkorb gleichzeitig bearbeitet werden können. Kombi-Geräte vereinen beide Funktionen.
Strahlgeräte enthalten Vorratsbehälter (Strahltanks) für ein oder mehrere unterschiedliche Strahlmittel (unterschiedlicher Körnung). Moderne Geräte sind häufig modular aufgebaut und können bei Bedarf einfach um weitere Strahltanks für Zusatzanwendungen erweitert werden. Die Identifizierung und Zuordnung von Strahlmittel, Strahlgriffel/-düse und zugehörigen Bedienelementen wird durch die Verwendung von Farbcodierungen erleichtert.
 Ein Strahlgerät
Ein Strahlgerät
Das Strahlmittel wird mit (vorzugsweise gefilterter, öl- und wasserfreier) Druckluft als Strahl durch eine feine Düse aus sehr widerstandsfähigem Werkstoff (etwa Borkarbid) auf die zu bearbeitende Oberfläche gelenkt. Bei guter Fokussierung des Strahls ist die Arbeitspräzision erhöht, gleichzeitig sinkt der Materialverbrauch. Die Strahlkammer bildet einen abgeschlossenen Arbeitsraum. Verwendetes Strahlmittel wird aufgefangen, durch Filtersysteme und Absaugungen einer Raumluftkontamination vorgebeugt. Mit Abscheidern werden Verunreinigungen des Strahlmittels entfernt.
Glasscheiben (die Lebensdauer wird durch optionale Schutzgitter erhöht), Beleuchtung und ergänzende Lupensysteme führen zu guter Sicht. Im Gerätegehäuse fest montierte Handschuhe (Stulpen) ermöglichen das Manipulieren von Werkstücken. Die Auslösung des Strahlvorganges erfolgt häufig über Fußschalter, um die Hände freizuhalten.
Entscheidend für ein optimales Abstrahlergebnis in möglichst kurzer und damit wirtschaftlicher Bearbeitungszeit ist die genaue Abstimmung von Strahldruck, Partikelgröße des Strahlmittels sowie Abstand und Winkel der Düse in Bezug auf das abzustrahlende Objekt.
Moderne Strahlgeräte sind universell einsetzbar für alle Anwendungsbereiche, wie etwa die Entfernung von Einbettmasseresten und Metalloxiden, das Anrauen zur Schaffung retentiver Oberflächen, Glanzstrahlen oder Mattstrahlen, Verdichtung von Metalloberflächen, aber auch spezielle Anwendungen wie die Kaltsilanisierung zur Beschichtung von Oberflächen im RocatecTM-System.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| bone remodeling | Knochenremodellation, Knochenumbau, knöcherne Remodelling, Knochenremodelling |
Focus text of the month
Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication… Root canal posts are inserted centrally into adequately long, straight sections of devitalised, root-filled teeth which show no pathological findings either clinically or radiologically. Severe vertical and horizontal structure loss from the clinical crown is an indication for root canal posts. The preferred method is generally to insert the root canal post, so that it (by predrilling with ascending diameters) virtually fills the prepared post site and fits close to the dentine wall. That section of the root canal post in the root should be at least as long as the crown restoration, leaving a few millimetres of the root canal filling to seal the apex. Isolated concepts have also been developed with smooth metal posts projecting apically beyond the tooth and intended for anchoring in the bone (transdental fixation).
Restoration with a temporary post is seldom practical due to the increased fracture and reinfection rate; a definitive root canal post should be inserted as early as possible.
Customised root canal posts (often made from precious metal alloys), cast after waxing up directly in the root canal or indirectly after taking an impression of the root canal lumen (using burnout posts), can also be used for filling lumina with oval or irregular cross sections, as well as two or three divergent canals each fitted with a post inserted, if necessary, through the opening of another canal. The core build-up(s), or even the entire crown (historically: post crown) can be integrated. |
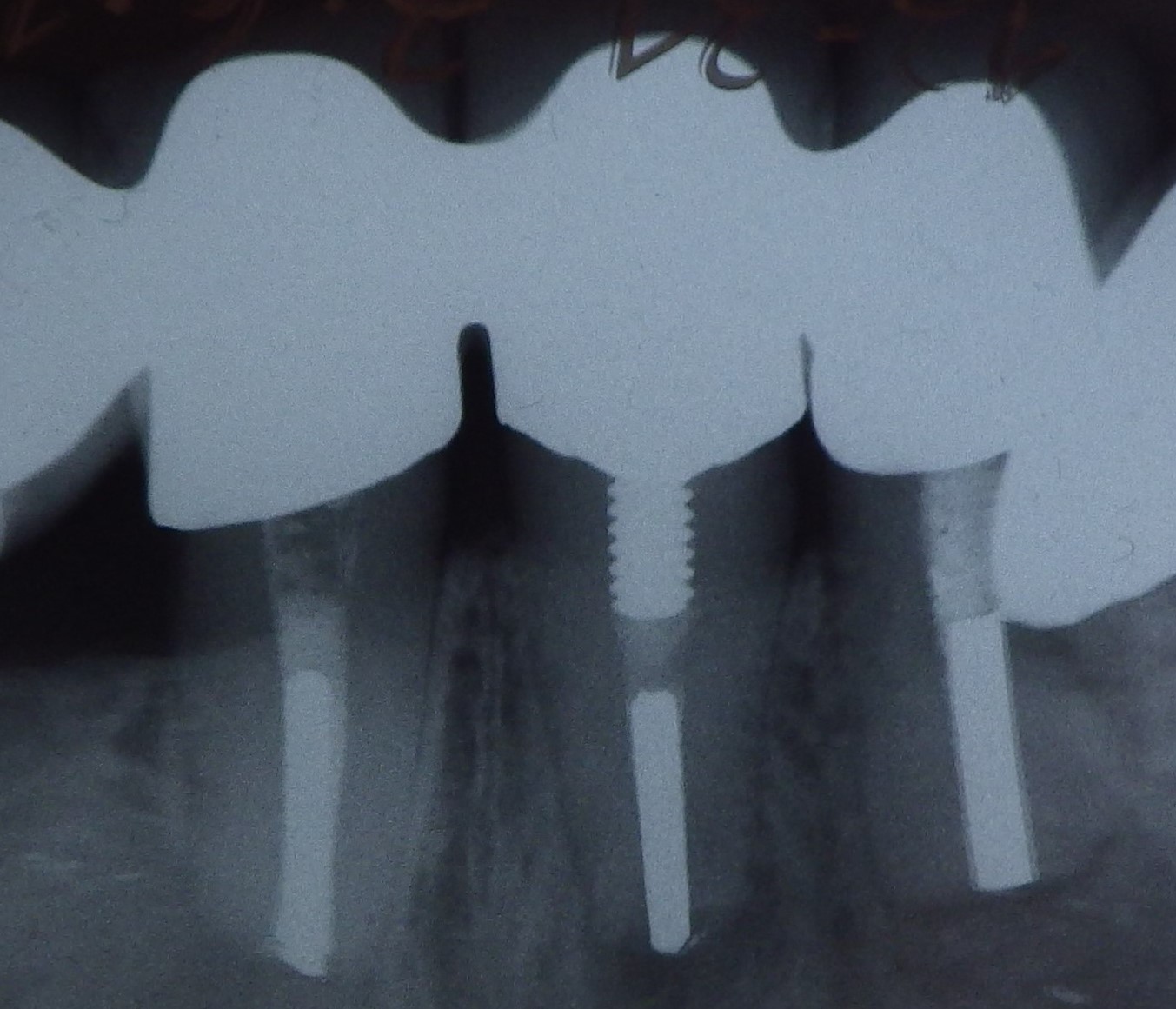 Three different root canal posts
Three different root canal posts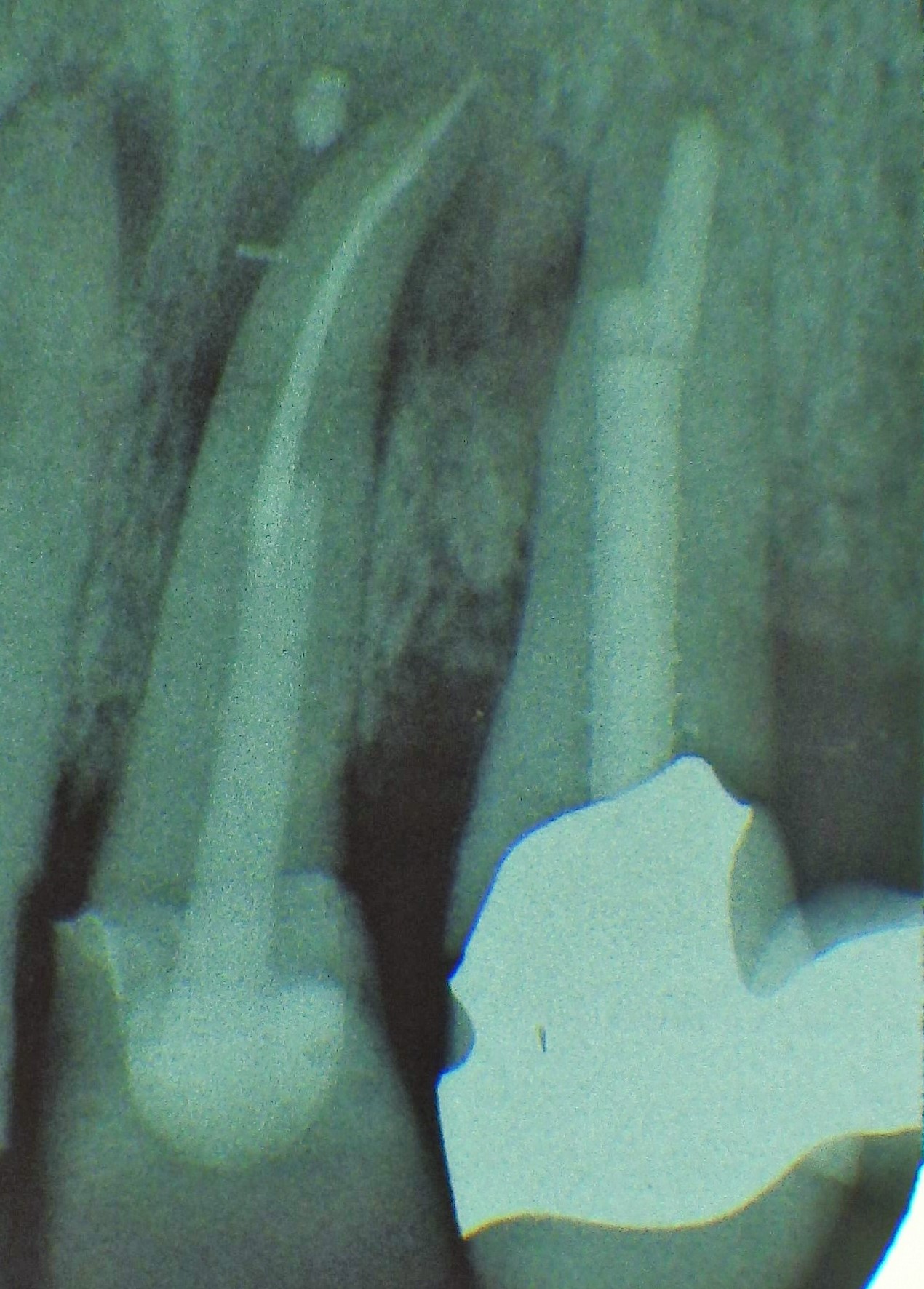 Tooth 14 conical and smooth, tooth 13 cylindrical and threaded
Tooth 14 conical and smooth, tooth 13 cylindrical and threaded