Sleep apnoea
Sleep apnoea
Sleep apnoea syndrome (SAS, prevalence approximately 5%, more men than women, increases with increasing age) is one of the sleep-related disorders (SRD), more specifically, sleep-related breathing disorders (SRBD).
Compared with healthy sleep, there is a great increase in breathing cessations (AHI = apnoea/hypopnoea index > 10 per hour), in the form of complete apnoea or reductions in airflow (hypopnoea). Central nervous system causes are rarer than the much more common OSA (obstructive sleep apnoea) of local (peripheral) origin. This itself causes central cessations, so mixed forms often occur (approx. 90%). OSAS (obstructive sleep apnoea syndrome) is nearly always associated with heavy snoring that disturbs other sleepers. The interaction of a number of factors, such as supine sleeping position, slack pharyngeal musculature, especially involving the soft palate and uvula and also the hypopharynx (e.g. due to alcohol consumption, sleeping pills), physiological and pathological anatomy (obstructed nasal breathing, enlarged tonsils, macroglossia, obesity) causes temporary complete obstruction of the airways during inspiration.
This causes a drop of about 4% in the blood's oxygen saturation, which is normally 95% to 100% so the oxygen supply to the tissues is impaired. If the episode lasts longer, hypercapnia (a rise in carbon dioxide level) may occur. This then triggers frequent "micro-arousals" via chemosensors, which often do not lead to full awakening; sleep is disturbed with shortened deep sleep phases and an overall reduction in sleep quality with lower relaxation and recovery, which can lead to an increased need for sleep and increased daytime tiredness, daytime somnolence (hypersomnia) and a tendency to fall asleep.
In the long term, apart from quality of life and energy levels, life expectancy is also affected as OSA is associated with high blood pressure, cardiac arrhythmias and depression and there is an increased tendency to stroke, heart attack and accidents.
The diagnosis can be confirmed by recording relevant parameters during sleep at home (cardiorespiratory polygraphy) or in hospital (polysomnography when the patient spends the night in the sleep laboratory); these include ECG, pulse oximetry, EEG, video recording, etc.
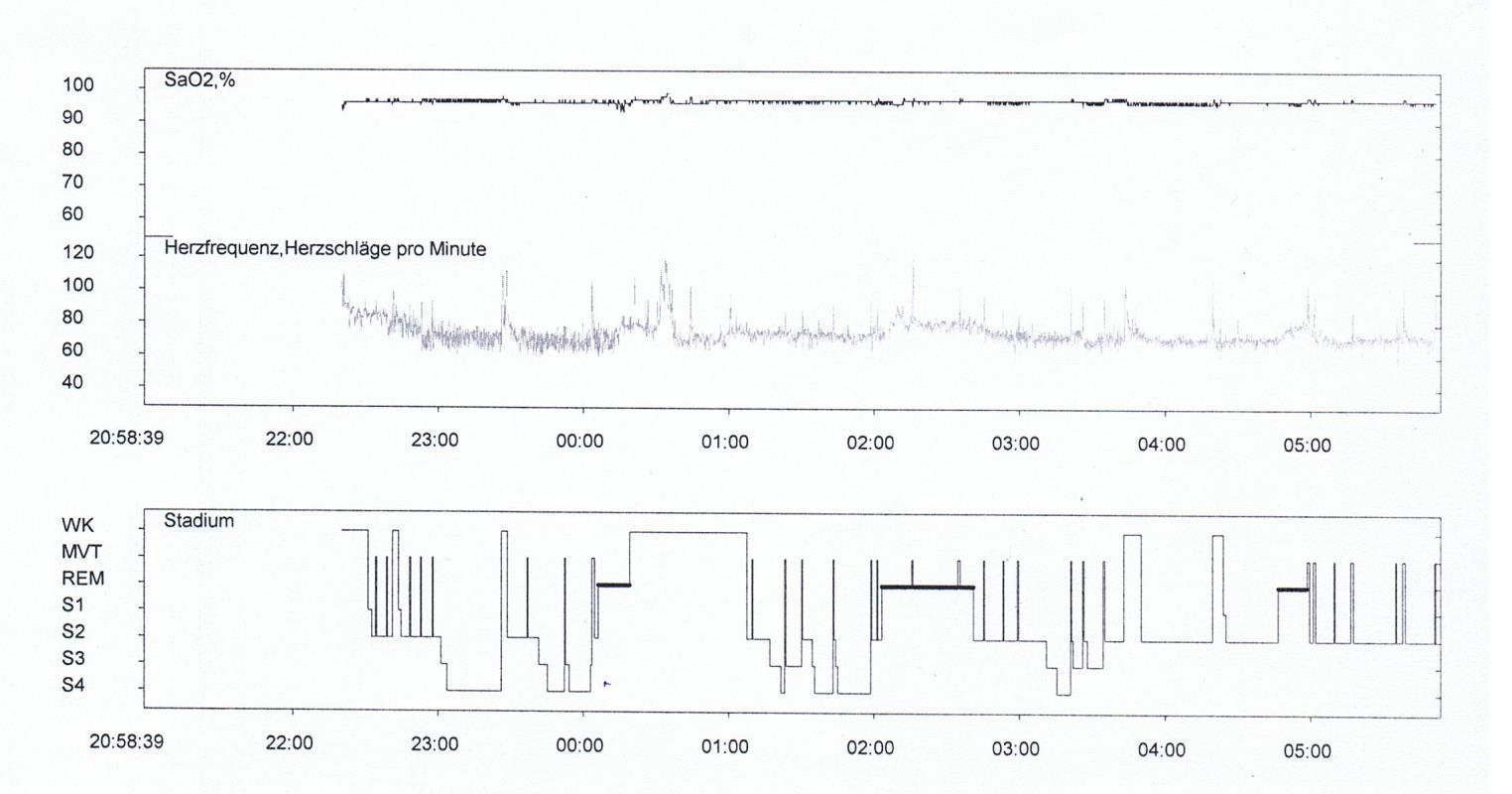 Polysomnogramme with hypnogramme
Polysomnogramme with hypnogramme
Various approaches are used in treatment, alone or in combination:
- Behavioural changes (abstinence from alcohol, lying on the side);
- Removable intraoral devices, usually bimaxillary and usually made in a dental laboratory ("anti-snoring appliance") to move the lower jaw ("protrusion splints") and/or the tongue forward. Thermoformed splints are often made separately for the upper and lower jaw and joined by special metal or plastic joints that allow certain movements.
- "Overpressure" ventilation with pure oxygen and continuous positive airway pressure (CPAP) via a face mask worn during the night.
- Invasive measures in severe cases: surgery to tighten or reduce the volume of tissues.
- Medications, by contrast, have shown little efficacy.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| arch expander | Erweiterungsapparatur |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration