Endodontie
Endodontie
Behandlungsformen, die den Zahninnenraum und den Bereich um die Wurzelspitze herum betreffen, werden zusammenfassend als Endodontie (endodontische Therapie) bezeichnet.
Endodontologen sind auf die E. spezialisierte Zahnärzte. Die E. ist ein Teilbereich der konservierenden Zahnheilkunde, dient also immer der Zahnerhaltung. Dazu gehören die (direkte) Überkappung eröffneter Pulpabereiche, die Wurzelspitzenresektion, vor allem aber die Wurzelkanalbehandlung. Sie ist indiziert bei irreversibler Pulpitis, Zerstörung der Pulpa durch Unfälle oder Infektionen sowie weiter bestehender oder erneut auftretender bakterieller Besiedelung bereits wurzelkanalbehandelter/wurzelkanalgefüllter Zähne (Revision).
Ziele sind zunächst die (praktisch) vollständige Elimination von erkranktem Gewebe, Fremdmaterial (etwa vorhandenem Wurzelkanalfüllmaterial), und Krankheitserregern aus dem Wurzelkanalsystem. Zu den chemischen Methoden gehört der Einsatz von antibakteriell und/oder gewebeauflösend wirkenden Lösungen (z.B. Chlorhexidin, EDTA, Natriumhypochlorit, Wasserstoffperoxid). Zur mechanischen Aufbereitung, d.h. also Ausräumung, Glättung, Reinigung und Erweiterung der (Haupt-)Wurzelkanäle werden maschinell oder manuell geführte Wurzelkanalinstrumente aus Stahl oder Nickel-Titan verwendet.
 Eröffnete Pulpakammer, Kofferdam
Eröffnete Pulpakammer, Kofferdam
Beide Verfahren in Kombination bilden die chemomechanische Aufbereitung. Medikamentöse Zwischeneinlagen (etwa mit Calciumhydroxid oder Chlor-Kampfer-Menthol) können zur weiteren Verminderung von Bakterien dienen. Abschließend werden die aufbereiteten Haupt-Wurzelkanäle obturiert, also mit einer Wurzelkanalfüllung (z.B. aus Guttaperchastiften und einem Wurzelkanalzement) ausgefüllt, abgedichtet und koronal mit einer adhäsiven Füllung und/oder einer Krone verschlossen.
 Wurzelkanalfüllungen 25, 26, 27
Wurzelkanalfüllungen 25, 26, 27
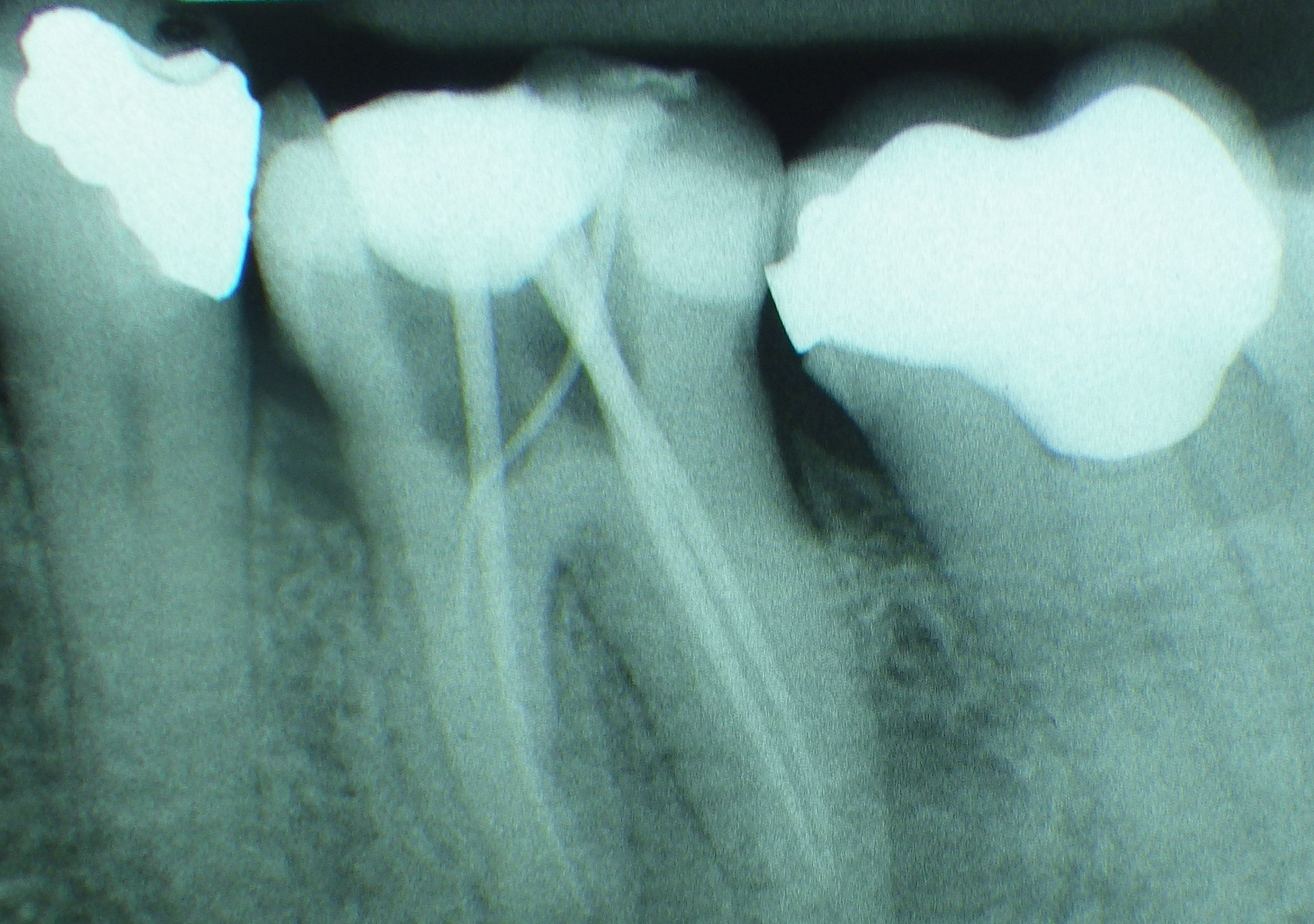 Masterpoint-Einzelröntgenaufnahme
Masterpoint-Einzelröntgenaufnahme
Im Endergebnis soll der behandelte Zahn langfristig beschwerdefrei/symptomlos sein und pathologische Veränderungen des apikalen Alveolarknochens ausbleiben oder (im Röntgenbild erkennbar) ausheilen. Die Erfolgswahrscheinlichkeit endodontischer Behandlungen. Sie wurde in den letzten beiden Jahrzehnten insbesondere durch zunehmenden Einsatz von Operationsmikroskopen und mikrochirurgischen Methoden deutlich erhöht und wird heute meist mit 90 % angegeben. Hinzu kommen Erfolge bei der Deckung von (auch iatrogenen) Perforationen oder der Entfernung abgebrochener Instrumente oder zementierter Stifte aus dem Wurzelkanalsystem.
Want to give it a try ...
... or need professional advice?
Get in touch with us or click Contact.
Word of the day
| English | German |
|---|---|
| attachment apparatus | Zahnhalteapparat, Parodont, Parodontium, Zahnbett, Desmodont, Desmodontium, Wurzelhaut, Wurzelperiost |
Focus text of the month
Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic… Composites also composite (from the Latin componere = to compose) are tooth-coloured filling materials with plastic properties used in dental treatment. In lay terms they are often referred to as plastic fillings, also erroneously sometimes confused with ceramic fillings due to their tooth colour. After being placed in a cavity they cure chemically or by irradiating with light or a combination of the two (dual-curing). Nowadays, composites are also used as luting materials. The working time can be regulated with light-curing systems, which is a great advantage both when placing fillings and during adhesive luting of restorations. Dual-curing luting materials are paste/paste systems with chemical and photosensitive initiators, which enable adequate curing, even in areas in which light curing is not guaranteed or controllable. Composites were manufactured in 1962 by mixing dimethacrylate (epoxy resin and methacrylic acid) with silanized quartz powder (Bowen 1963). Due to their characteristics (aesthetics and advantages of the adhesive technique) composite restorations are now used instead of amalgam fillings.
The material consists of three constituents: the resin matrix (organic component), the fillers (inorganic component) and the composite phase. The resin matrix mainly consists of Bis-GMA (bisphenol-A-glycidyldimethacrylate). As Bis-GMA is highly viscous, it is mixed in a different composition with shorter-chain monomers such as, e.g. TEGDMA (triethylene glycol dimethacrylate). The lower the proportion of Bis-GMA and the higher the proportion of TEGDMA, the higher the polymerisation shrinkage (Gonçalves et al. 2008). The use of Bis-GMA with TEGDMA increases the tensile strength but reduces the flexural strength (Asmussen & Peutzfeldt 1998). Monomers can be released from the filling material. Longer light-curing results in a better conversion rate (linking of the individual monomers) and therefore to reduced monomer release (Sideriou & Achilias 2005) The fillers are made of quartz, ceramic and/ or silicon dioxide. An increase in the amount of filler materials results in decreases in polymerisation shrinkage, coefficient of linear expansion and water absorption. In contrast, with an increase in the filler proportion there is a general rise in the compressive and tensile strengths, modulus of elasticity and wear resistance (Kim et al. 2002). The filler content in a composite is also determined by the shape of the fillers.
Composite restorations Conclusion |
 Minimally-invasive preparation and
Minimally-invasive preparation and  indiscernible composite restoration
indiscernible composite restoration